

Liberal Versus Restrictive Transfusion in Acute Brain Injury: A Systematic Review and Meta-Analysis
- PMID: 40491611
- PMCID: PMC12148049
- DOI: 10.7759/cureus.83847
Liberal Versus Restrictive Transfusion in Acute Brain Injury: A Systematic Review and Meta-Analysis
Abstract
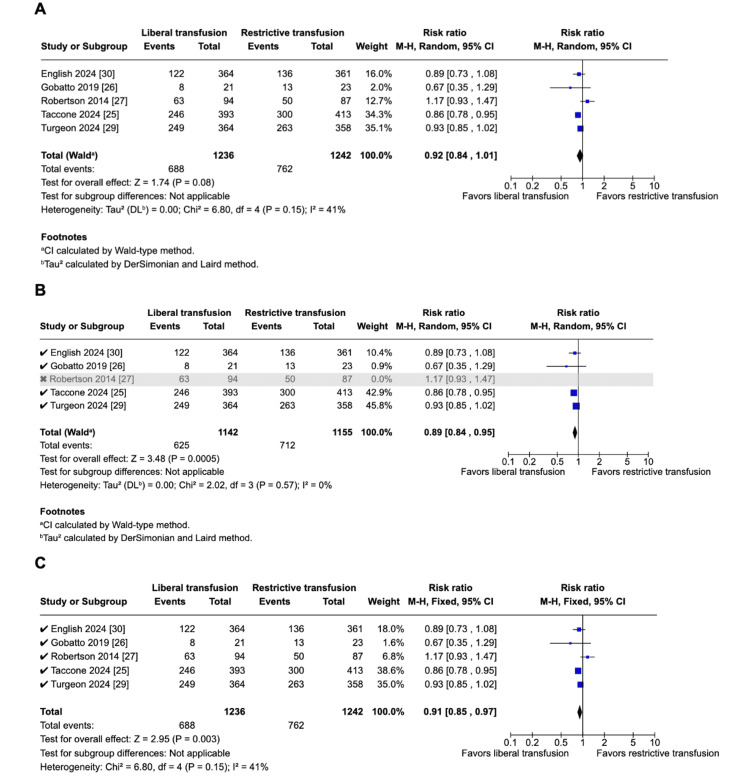
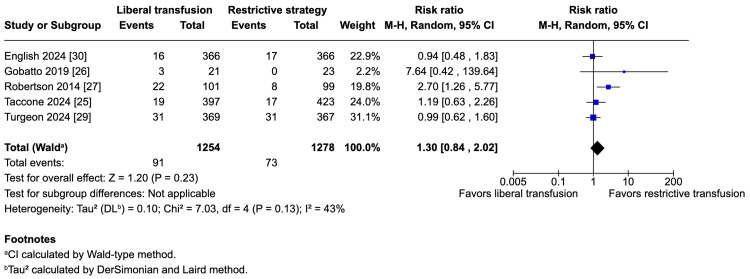
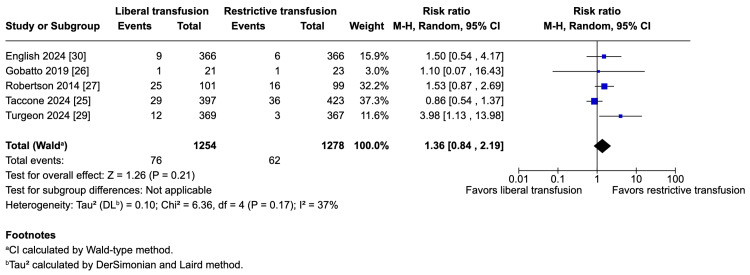
Oxygen is critical for neurological function and survival, particularly in acute brain injury. Although transfusion at higher thresholds theoretically provides improved oxygen delivery to neurons, there is an associated risk of allogeneic reactions and increased utilization of limited blood resources. Conversely, although a lower threshold conserves resources, it may increase the risk of neuronal oxygen deprivation. The optimal transfusion strategy for patients with acute brain injury remains unclear. This systematic review and meta-analysis aimed to compare the efficacy and safety of liberal (hemoglobin threshold ≤10 g/dL) versus restrictive (≤8 g/dL) transfusion strategies in patients with acute brain injury (traumatic brain injury (TBI), subarachnoid hemorrhage, or intracranial hemorrhage), synthesizing evidence from randomized controlled trials (RCTs). We searched the PubMed, Excerpta Medica database (Embase), and the Cochrane Central Register of Controlled Trials (CENTRAL) databases to identify RCTs comparing restrictive and liberal transfusion strategies in patients with acute brain injury. Eligible trials reported outcomes including (1) unfavorable neurological outcomes defined as a score ≤5 on the Glasgow Outcome Scale Extended (GOSE) at six months, (2) mortality, (3) acute respiratory distress syndrome (ARDS), and (4) infections. Statistical heterogeneity was assessed using I² statistics. To account for statistical heterogeneity, a random-effects model was used to analyze all outcomes. We included six RCTs comprising 2,645 patients, of whom 1,303 (49.2%) were randomized to a liberal transfusion strategy. A reduction in unfavorable neurological endpoints (55.7% vs. 61.4%; risk ratios (RR) 0.92; 95% CI 0.84-1.01) was observed in the liberal group, although this difference was not statistically significant. In sensitivity analyses of unfavorable neurologic outcomes, statistical significance was achieved by removing a single paper (54.7% vs. 61.6%; RR 0.89; 95% CI 0.84-0.95) or by employing a fixed-effects model (RR 0.91; 95% CI 0.85-0.97). This meta-analysis suggests that there is no substantial difference in outcomes between a liberal and a restrictive transfusion strategy in patients with acute brain injury. While our primary analysis showed no statistically significant difference between strategies, sensitivity analyses suggested a potential benefit of liberal transfusion in reducing unfavorable neurologic outcomes. However, given the non-significant primary results and the importance of blood conservation, a restrictive strategy may be reasonable until further evidence emerges.
Keywords: acute brain injury; liberal transfusion; restrictive transfusion; subarachnoid hemorrhage; traumatic brain injury.
Copyright © 2025, Bena Nnang et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Liberal vs restrictive transfusion strategy for acute brain injury: A meta-analysis with trial sequential analysis of randomized clinical trials.Anaesth Crit Care Pain Med. 2025 Jun 13:101566. doi: 10.1016/j.accpm.2025.101566. Online ahead of print. Anaesth Crit Care Pain Med. 2025. PMID: 40518044
-
Efficacy of restrictive versus liberal transfusion strategies in patients with traumatic brain injury: a systematic review and meta-analysis of randomized controlled trials.Ann Intensive Care. 2024 Nov 28;14(1):177. doi: 10.1186/s13613-024-01411-1. Ann Intensive Care. 2024. PMID: 39607477 Free PMC article. Review.
-
Liberal vs. restrictive transfusion strategies for acute brain injury: a systematic review and frequentist-Bayesian meta-analysis.Intensive Care Med. 2025 Feb;51(2):353-363. doi: 10.1007/s00134-025-07807-2. Epub 2025 Feb 17. Intensive Care Med. 2025. PMID: 39961845
-
Restrictive vs Liberal Transfusion Strategy in Patients With Acute Brain Injury: The TRAIN Randomized Clinical Trial.JAMA. 2024 Nov 19;332(19):1623-1633. doi: 10.1001/jama.2024.20424. JAMA. 2024. PMID: 39382241 Free PMC article. Clinical Trial.
-
Transfusion Thresholds and Neurological Functional Outcome After Acute Brain Injury: An Updated Systematic Review and Meta-Analysis of Randomized Clinical Trials.J Clin Med. 2025 May 16;14(10):3487. doi: 10.3390/jcm14103487. J Clin Med. 2025. PMID: 40429483 Free PMC article. Review.
References
-
- Estimating the global incidence of traumatic brain injury. Dewan MC, Rattani A, Gupta S, et al. J Neurosurg. 2019;130:1080–1097. - PubMed
-
- Williamson C, Venkatakrishna R. UpToDate. Waltham, MA: UpToDate; 2025. Traumatic brain injury: epidemiology, classification, and pathophysiology.
-
- Measuring the burden of secondary insults in head-injured patients during intensive care. Jones PA, Andrews PJ, Midgley S, et al. https://pubmed.ncbi.nlm.nih.gov/8298263/ J Neurosurg Anesthesiol. 1994;6:4–14. - PubMed
-
- The incidence and impact of secondary cerebral insults on outcome after aneurysmal subarachnoid hemorrhage. Doerfler S, Faerber J, McKhann GM, et al. World Neurosurg. 2018;114:0–94. - PubMed
Publication types
LinkOut - more resources
Full Text Sources