

Evaluating Surgical Trends and Outcomes in Stress Urinary Incontinence: A Clinical Audit at a District General Hospital
- PMID: 40491644
- PMCID: PMC12146218
- DOI: 10.7759/cureus.83815
Evaluating Surgical Trends and Outcomes in Stress Urinary Incontinence: A Clinical Audit at a District General Hospital
Abstract
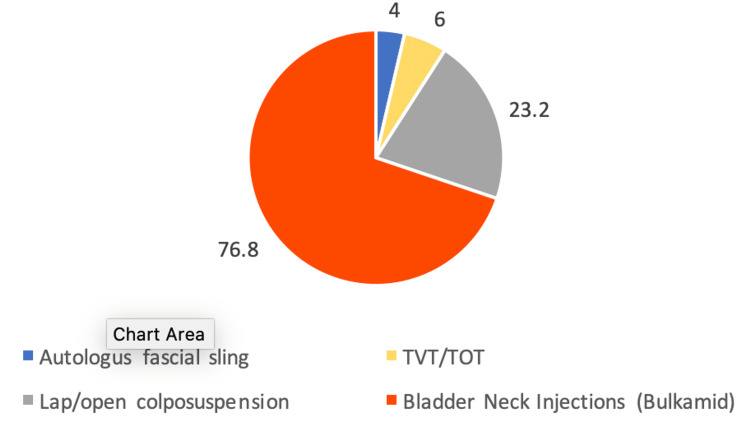
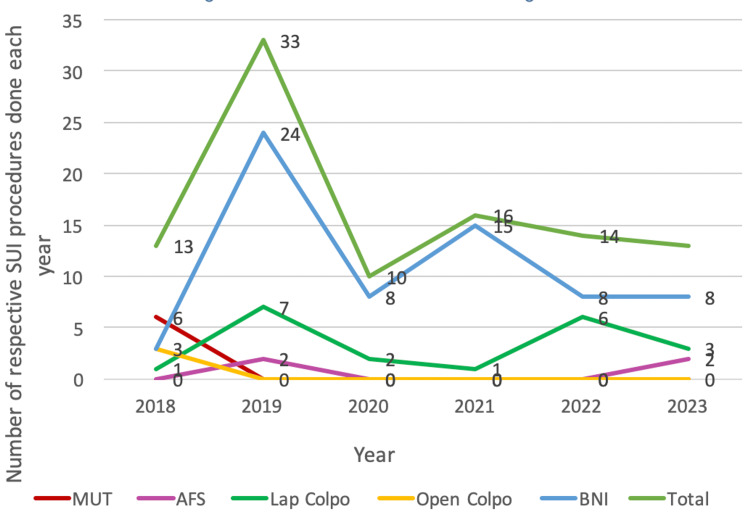
Stress urinary incontinence (SUI) significantly impairs quality of life. This retrospective audit aimed to evaluate surgical treatment patterns and outcomes for SUI at a district general hospital between 2018 and 2023 and to compare them with national benchmarks from the third British Society of Urogynaecology (BSUG) report in 2020-21. Data from 99 patients were collected from the BSUG database and hospital electronic records, following clinical audit department approval. The mean age of patients undergoing surgery was 50 years. In 2018, mid-urethral tape was the most commonly performed procedure (46.2%); however, following the UK-wide suspension of vaginal mesh procedures that year, there was a notable shift towards alternative surgeries. Bladder neck injections (BNIs), colposuspension (open and laparoscopic), and autologous fascial sling (AFS) procedures all increased in frequency, mirroring national trends. BNIs became the predominant procedure, accounting for 76.8% of cases, with over 80% performed on an outpatient basis. Reported cure rates, when compared to national figures, were AFS (100% vs. 94%), laparoscopic colposuspension (71.4% vs. 84%), BNIs (66% vs. 60%), and open colposuspension (33.3% vs. 81%). Bladder injuries occurred in 17.3% of colposuspension cases, significantly higher than the national average of 2.7%. Additionally, prolonged catheterisation (>10 days) was noted in 29% of colposuspension cases, compared to 7.1% nationally. These elevated complication rates may reflect the procedural learning curve, as laparoscopic colposuspension was only recently introduced at the center. The audit highlights evolving surgical trends and outcomes in the management of SUI following the national mesh pause, with a shift toward non-mesh alternatives. Further audits with long-term follow-up and larger sample sizes are recommended to assess the safety, efficacy, and patient-reported outcomes of these procedures.
Keywords: autologous fascial sling; bladder neck injection; colposuspension; mesh pause; stress urinary incontinence; surgical outcomes; urogynaecology audit.
Copyright © 2025, Kaur et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Clinical Audit and Effectiveness Department, Wrightington, Wigan and Leigh NHS Foundation Trust issued approval Not applicable. This audit was registered and approved by the NHS Trust's Quality Improvement and Audit Department. A review by the Trust's Research Committee and further confirmation via the “Is My Study Research?” tool (hra-decisiontools.org.uk) indicated that formal NHS Research Ethics Committee approval was unnecessary. Informed written consent was not required because data entry into the BSUG system is part of standard practice and consent for data recording is routinely obtained at the time of care. All data were entered into a password-protected Excel spreadsheet on a secure Trust computer. The only patient identifier used was the hospital number, which was necessary for tracking follow-up and readmissions. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
National BSUG audit of stress urinary incontinence surgery in England.Int Urogynecol J. 2019 Aug;30(8):1337-1341. doi: 10.1007/s00192-018-3705-4. Epub 2018 Jul 11. Int Urogynecol J. 2019. PMID: 29995163 Free PMC article.
-
[Recurrent stress urinary incontinence in women: results of surgical reinterventions].Urologiia. 2025 May;(2):11-15. Urologiia. 2025. PMID: 40377575 Russian.
-
The Midurethral Fascial "Sling on a String": An Alternative to Midurethral Synthetic Tapes in the Era of Mesh Complications.Eur Urol. 2018 Aug;74(2):191-196. doi: 10.1016/j.eururo.2018.04.031. Epub 2018 May 24. Eur Urol. 2018. PMID: 29803585
-
Traditional suburethral sling operations for urinary incontinence in women.Cochrane Database Syst Rev. 2020 Jan 28;1(1):CD001754. doi: 10.1002/14651858.CD001754.pub5. Cochrane Database Syst Rev. 2020. PMID: 31990055 Free PMC article.
-
Laparoscopic colposuspension for urinary incontinence in women.Cochrane Database Syst Rev. 2019 Dec 10;12(12):CD002239. doi: 10.1002/14651858.CD002239.pub4. Cochrane Database Syst Rev. 2019. PMID: 31821550 Free PMC article.
References
-
- Medical resource utilisation and cost of care for women seeking treatment for urinary incontinence in an outpatient setting. Examples from three countries participating in the PURE study. Papanicolaou S, Pons ME, Hampel C, et al. Maturitas. 2005;52 Suppl 2:0–47. - PubMed
-
- The cost of clinically significant urinary storage symptoms for community dwelling adults in the UK. Turner DA, Shaw C, McGrother CW, Dallosso HM, Cooper NJ. BJU Int. 2004;93:1246–1252. - PubMed
-
- Stress incontinence in women. Wu JM. N Engl J Med. 2021;384:2428–2436. - PubMed
LinkOut - more resources
Full Text Sources