

Deep Learning in Digital Breast Tomosynthesis: Current Status, Challenges, and Future Trends
- PMID: 40491967
- PMCID: PMC12146671
- DOI: 10.1002/mco2.70247
Deep Learning in Digital Breast Tomosynthesis: Current Status, Challenges, and Future Trends
Abstract
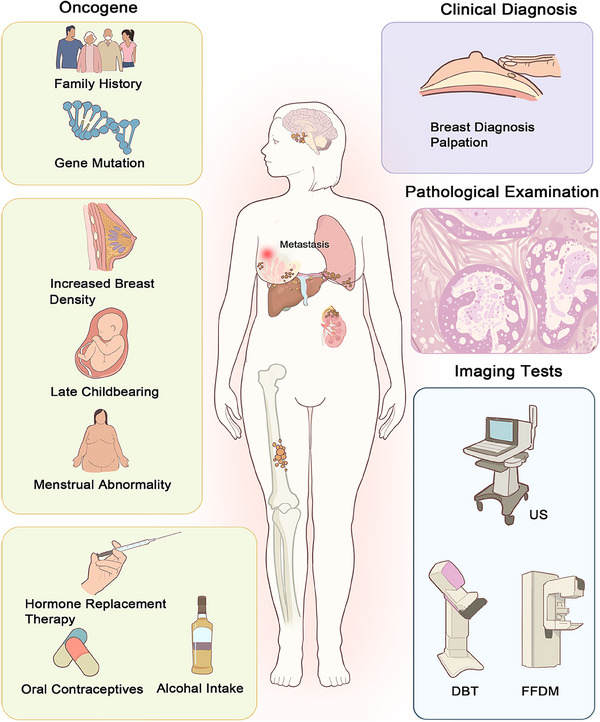
The high-resolution three-dimensional (3D) images generated with digital breast tomosynthesis (DBT) in the screening of breast cancer offer new possibilities for early disease diagnosis. Early detection is especially important as the incidence of breast cancer increases. However, DBT also presents challenges in terms of poorer results for dense breasts, increased false positive rates, slightly higher radiation doses, and increased reading times. Deep learning (DL) has been shown to effectively increase the processing efficiency and diagnostic accuracy of DBT images. This article reviews the application and outlook of DL in DBT-based breast cancer screening. First, the fundamentals and challenges of DBT technology are introduced. The applications of DL in DBT are then grouped into three categories: diagnostic classification of breast diseases, lesion segmentation and detection, and medical image generation. Additionally, the current public databases for mammography are summarized in detail. Finally, this paper analyzes the main challenges in the application of DL techniques in DBT, such as the lack of public datasets and model training issues, and proposes possible directions for future research, including large language models, multisource domain transfer, and data augmentation, to encourage innovative applications of DL in medical imaging.
Keywords: deep learning; digital breast tomosynthesis; early breast cancer screening; medical image analysis; public database.
© 2025 The Author(s). MedComm published by Sichuan International Medical Exchange & Promotion Association (SCIMEA) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Jemal A., Bray F., Center M. M., Ferlay J., Ward E., and Forman D., “Global Cancer Statistics,” CA: A Cancer Journal for Clinicians 61, no. 2 (2011): 69–90. - PubMed
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R. L., Torre L. A., and Jemal A., “Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA: A Cancer Journal for Clinicians 68, no. 6 (2018): 394–424. - PubMed
-
- Bray F., Laversanne M., Sung H., et al., “Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA: A Cancer Journal for Clinicians 74, no. 3 (2024): 229–263. - PubMed
Publication types
LinkOut - more resources
Full Text Sources