

This is a preprint.
Estimated Impact of Model-Guided Venous Thromboembolism Prophylaxis versus Physician Practice
- PMID: 40492076
- PMCID: PMC12148274
- DOI: 10.1101/2025.05.29.25328593
Estimated Impact of Model-Guided Venous Thromboembolism Prophylaxis versus Physician Practice
Abstract
Background: The American Society of Hematology (ASH) recommends assessing venous thromboembolism (VTE) and major bleeding risk to optimize pharmacological VTE prophylaxis for medical inpatients. However, the clinical utility of model-guided approaches remains unknown.
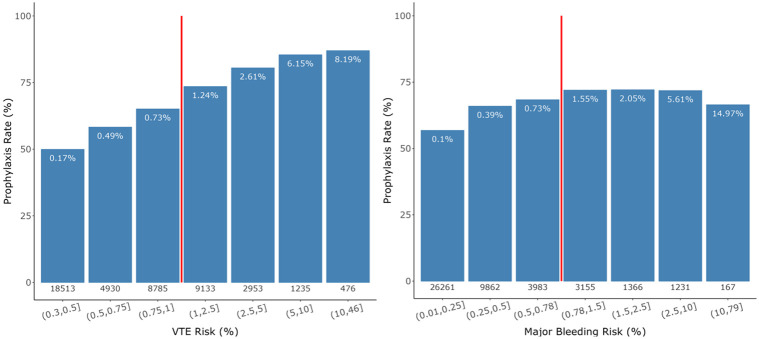
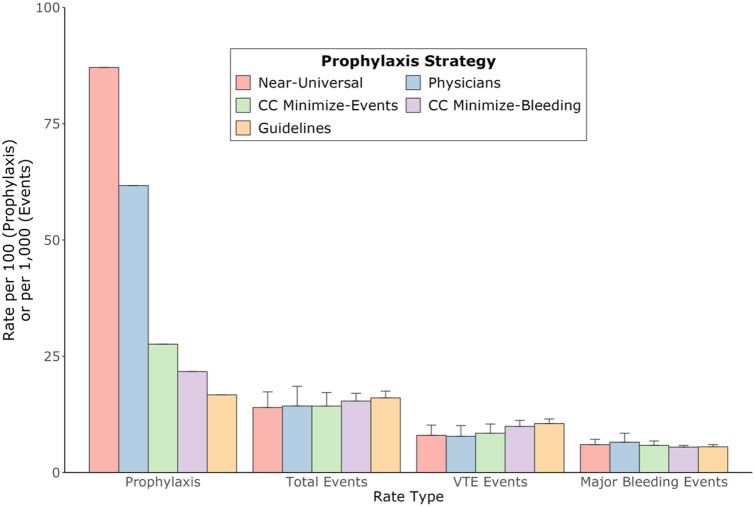
Methods: Our objective was to estimate differences in VTE and major bleeding event rates and efficiency with prophylaxis guided by risk models versus prophylaxis based on physician judgment. Patients were adults admitted to one of 10 Cleveland Clinic hospitals between December 2017 and January 2020. We compared physician practice with hypothetical prophylaxis recommended by model-based prophylaxis strategies, including ASH-recommended risk scores (Padua and IMPROVE) and locally derived Cleveland Clinic risk prediction models. For each strategy we quantified the prophylaxis rate, VTE and major bleeding rates, and the incremental number-needed-to-treat (NNT) to prevent one event (VTE or bleeding).
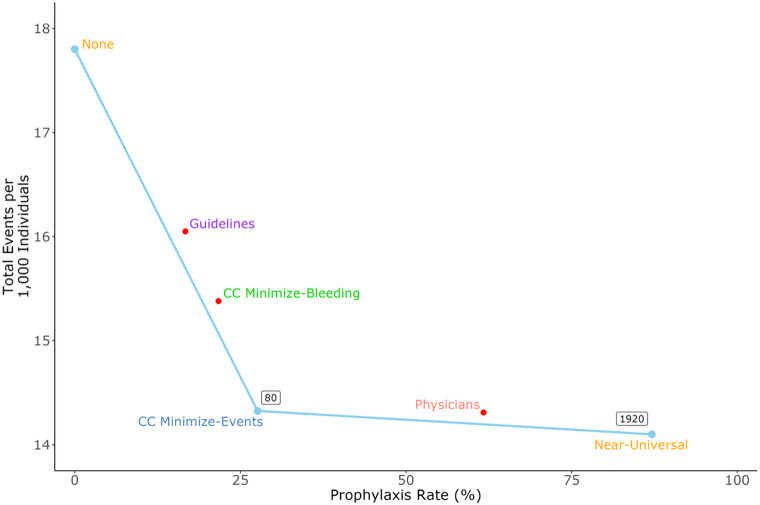
Results: Physicians prescribed prophylaxis to 62% of patients whereas model-based strategies recommended prophylaxis for 17-87%. Model-guided prophylaxis produced more VTEs and fewer major bleeds than physicians, but total events varied among strategies. Overall, per 1,000 patients, model-based strategies produced 14.0-16.1 events compared with 14.3 for physicians. The Padua/IMPROVE models recommended prophylaxis for the fewest patients but caused the most total events. The most efficient model-based strategy recommended prophylaxis to 28% of patients with an incremental NNT (relative to no prophylaxis) of 80. Compared to physicians, it reduced prophylaxis by 55% and total events by 0.14%.
Conclusions: Physicians often prescribed inappropriate prophylaxis, highlighting the need for decision support. A model-based strategy maximized efficiency, reducing both events and prophylaxis relative to physicians.
Keywords: clinical decision support systems; clinical utility; hemorrhage; heparin; risk assessment; venous thromboembolism.
Conflict of interest statement
Disclosures Authors have no conflicts of interest to declare.
Figures
Similar articles
-
Standard- versus extended-duration anticoagulation for primary venous thromboembolism prophylaxis in acutely ill medical patients.Cochrane Database Syst Rev. 2024 Dec 4;12(12):CD014541. doi: 10.1002/14651858.CD014541.pub2. Cochrane Database Syst Rev. 2024. PMID: 39629741
-
Pharmacological interventions for preventing venous thromboembolism in people undergoing bariatric surgery.Cochrane Database Syst Rev. 2022 Nov 22;11(11):CD013683. doi: 10.1002/14651858.CD013683.pub2. Cochrane Database Syst Rev. 2022. PMID: 36413425 Free PMC article.
-
Interventions for implementation of thromboprophylaxis in hospitalized patients at risk for venous thromboembolism.Cochrane Database Syst Rev. 2018 Apr 24;4(4):CD008201. doi: 10.1002/14651858.CD008201.pub3. Cochrane Database Syst Rev. 2018. PMID: 29687454 Free PMC article.
-
Neuromuscular electrical stimulation for the prevention of venous thromboembolism.Cochrane Database Syst Rev. 2017 Nov 21;11(11):CD011764. doi: 10.1002/14651858.CD011764.pub2. Cochrane Database Syst Rev. 2017. PMID: 29161465 Free PMC article.
-
Interventions for implementation of thromboprophylaxis in hospitalized medical and surgical patients at risk for venous thromboembolism.Cochrane Database Syst Rev. 2013 Jul 16;(7):CD008201. doi: 10.1002/14651858.CD008201.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2018 Apr 24;4:CD008201. doi: 10.1002/14651858.CD008201.pub3. PMID: 23861035 Updated.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous