

Perioperative fluid therapy impairs lymphatic pump function in male rats
- PMID: 40495298
- PMCID: PMC12151903
- DOI: 10.14814/phy2.70389
Perioperative fluid therapy impairs lymphatic pump function in male rats
Abstract
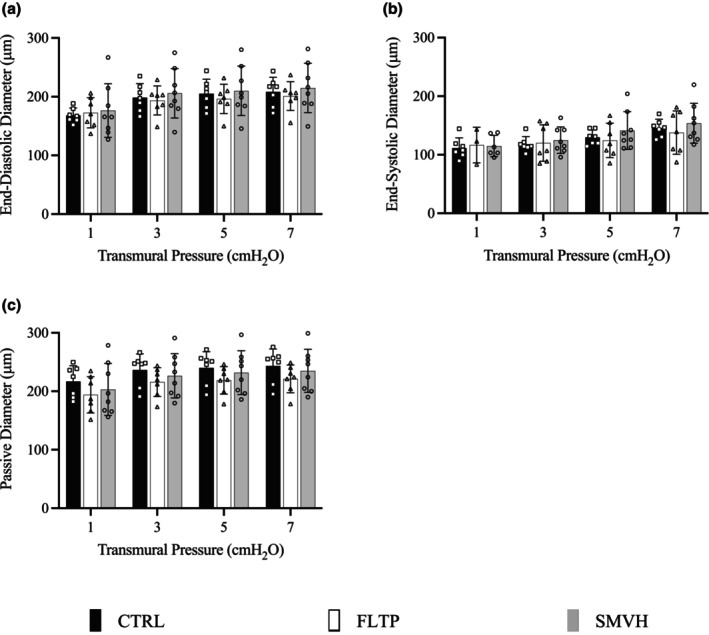
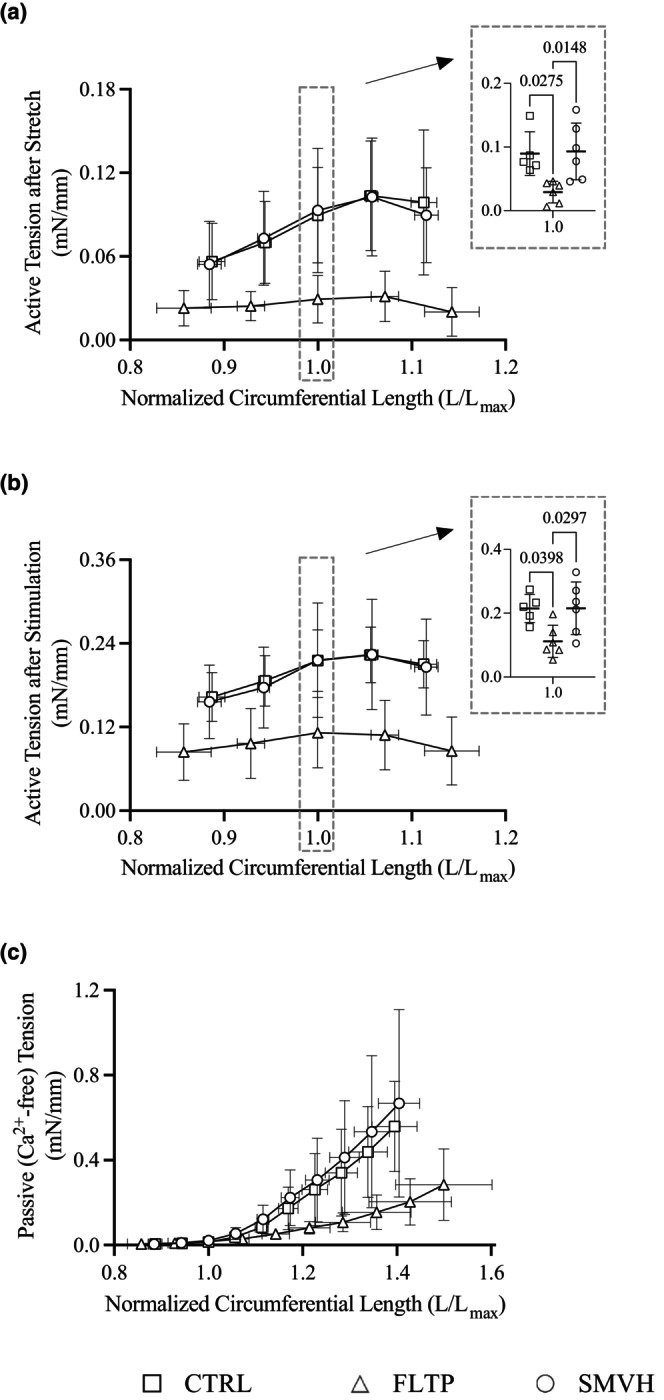
Because of its life-saving benefits, perioperative IV fluid therapy remains a cornerstone of medical treatment. However, it also induces sustained edemagenic stress. The resulting persistent interstitial edema-excessive fluid accumulation in the interstitium-significantly delays recovery and worsens patient outcomes. Therefore, to gain a detailed understanding of the lymphatic functional consequences of perioperative fluid therapy, this study aimed to test the hypothesis that perioperative IV fluid therapy compromises lymphatic pump function within 3 days after major surgery. Following a midline laparotomy, animals received IV fluid therapy over 48 h during recovery (FLTP). Three days post-surgery, mesenteric lymphatic vessels from FLTP and sham surgery (CTRL) animals were isolated, and lymphatic pump function was assessed in vitro. The transmural pressure-pump flow and circumferential length-wall tension relationships of FLTP vessels were altered-contraction frequency and normalized pump flow and active and passive wall tensions were significantly lower than CTRL. In vessels from another group of animals with surgically produced mesenteric venous hypertension to induce sustained edemagenic stress, only the pressure-pump flow relationship was altered similarly to FLTP. These results demonstrate the detrimental effects of perioperative fluid therapy on lymphatic pumping, which is essential for restoring interstitial fluid pressure and resolving edema and inflammation.
Keywords: enhanced recovery after surgery; goal‐directed fluid therapy; gut edema; intestinal dysfunction; resuscitation.
© 2025 The Author(s). Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this article.
Figures


References
-
- Amerini, S. , Ziche, M. , Greiner, S. T. , & Zawieja, D. C. (2004). Effects of substance P on mesenteric lymphatic contractility in the rat. Lymphatic Research and Biology, 2, 2–10. - PubMed
-
- Aukland, K. , & Reed, R. K. (1993). Interstitial‐lymphatic mechanisms in the control of extracellular fluid volume. Physiological Reviews, 73, 1–78. - PubMed
-
- Balogh, Z. , McKinley, B. A. , Cocanour, C. S. , Kozar, R. A. , Cox, C. S. , & Moore, F. A. (2003). Patients with impending abdominal compartment syndrome do not respond to early volume loading. American Journal of Surgery, 186, 602–607. - PubMed
-
- Balogh, Z. , McKinley, B. A. , Cocanour, C. S. , Kozar, R. A. , Holcomb, J. B. , Ware, D. N. , & Moore, F. A. (2002). Secondary abdominal compartment syndrome is an elusive early complication of traumatic shock resuscitation. American Journal of Surgery, 184, 538–543. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
