

Does geographical location impact the efficacy of oral antihypertensive therapy in pregnancy?
- PMID: 40495564
- PMCID: PMC12152777
- DOI: 10.4274/jtgga.galenos.2024.2024-1-8
Does geographical location impact the efficacy of oral antihypertensive therapy in pregnancy?
Abstract
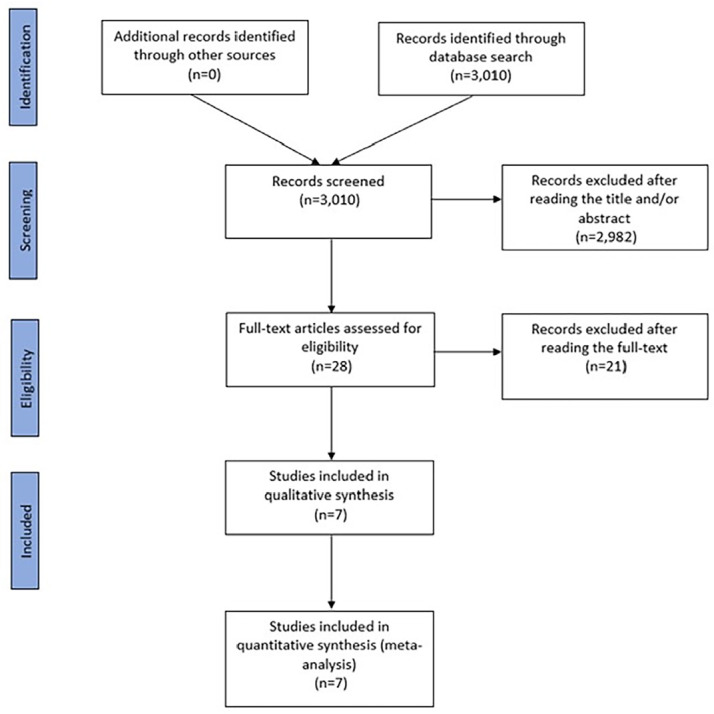
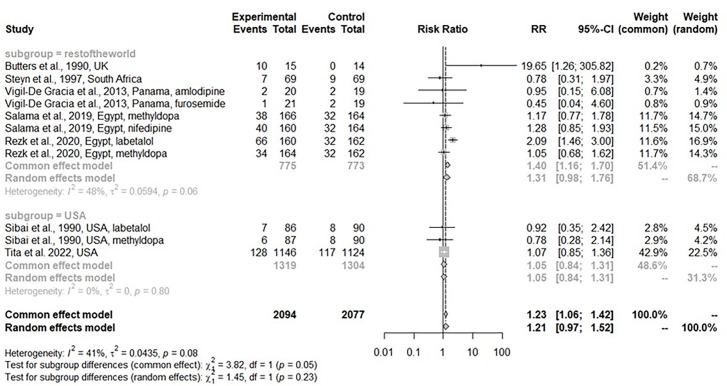
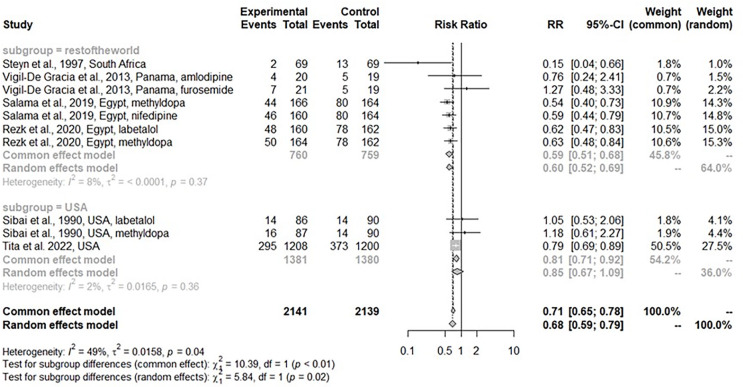
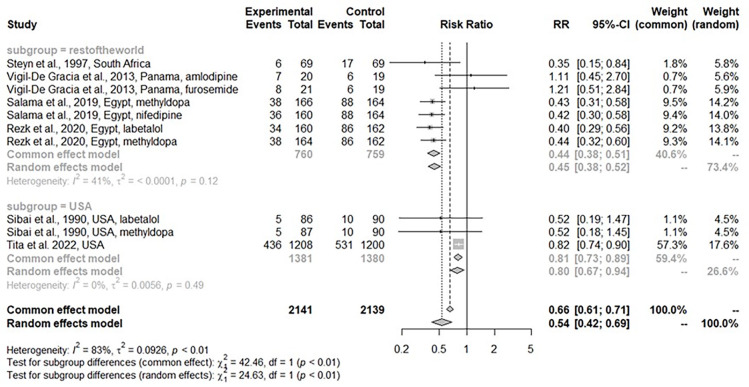
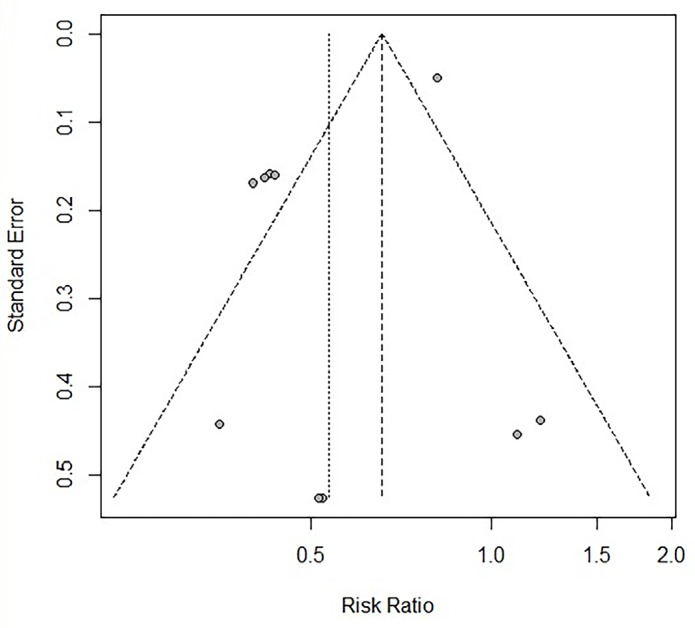
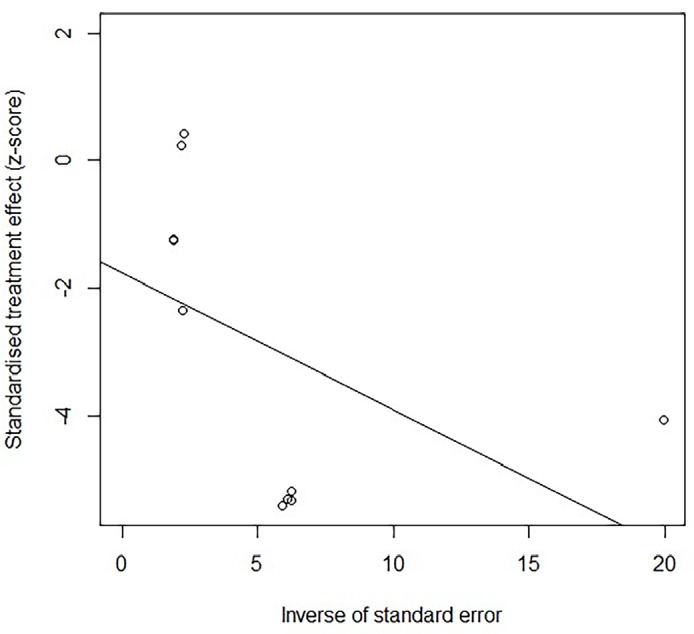
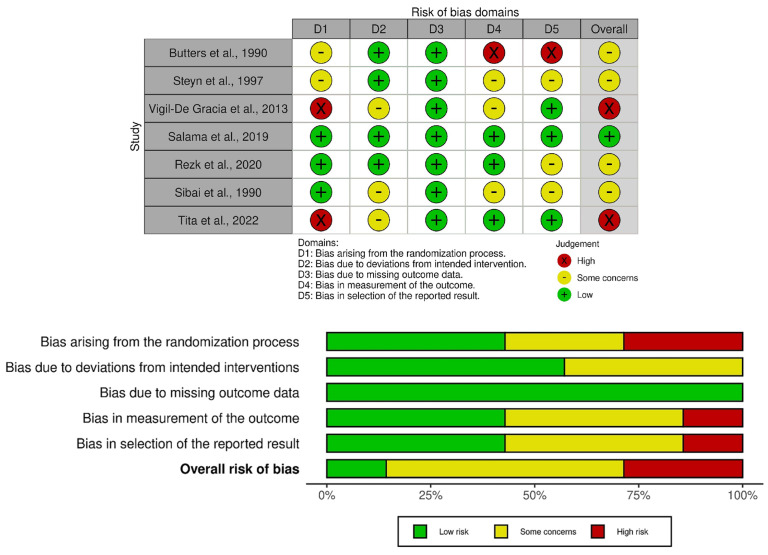
To assess the efficacy of anti-hypertensive medications during pregnancy according to race, ethnicity and geographical location as current evidence is not clear in this regard. A subgroup meta-analysis of randomized controlled trials was performed. The efficacy of oral medications for chronic hypertension in pregnancy by geographical location [United States of America (USA) vs. rest of the World] was investigated. The location was used as a surrogate of racial identification and differences in health care systems and availability of medications that might affect the efficacy of the treatment. The number of patients in each group experiencing the following outcomes: small for gestational age (SGA), preeclampsia, severe hypertension were compared. Seven studies were identified. Subgroup analysis revealed that medications did not affect the occurrence of SGA. In six studies, therapies were protective for preeclampsia in the rest of the world but not in USA (p=0.02). Therapies were protective for severe hypertension. Our findings suggest that location does not affect the efficacy of medication in treating chronic hypertension during pregnancy. Geographical location may serve as a surrogate for genetic characteristics of a population of interest. However, it can also be influenced by other factors such as the heterogeneity of populations such as the USA.
Keywords: Geographical location; hypertensive disorders of pregnancy; oral therapy; preeclampsia; pregnancy.
Copyright© 2025 The Author. Published by Galenos Publishing House on behalf of Turkish-German Gynecological Association.
Conflict of interest statement
Conflict of Interest: No conflict of interest is declared by the authors.
Figures
References
-
- Sisti G, Fochesato C, Elkafrawi D, Marcus B, Schiattarella A. Is blood pressure 120-139/80-89 mmHg before 20 weeks a risk factor for hypertensive disorders of pregnancy? A meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2023;284:66–75. - PubMed
-
- Leenen FH, Nwachuku CE, Black HR, Cushman WC, Davis BR, Simpson LM, et al. Clinical events in high-risk hypertensive patients randomly assigned to calcium channel blocker versus angiotensin-converting enzyme inhibitor in the antihypertensive and lipid-lowering treatment to prevent heart attack trial. Hypertension. 2006;48(3):374–84. doi: 10.1161/01.hyp.0000231662.77359.de. - DOI - PubMed
LinkOut - more resources
Full Text Sources