

Probability of sequelae following Campylobacter spp. infections: Update of systematic reviews and meta-analyses
- PMID: 40496789
- PMCID: PMC12039688
- DOI: 10.1002/puh2.145
Probability of sequelae following Campylobacter spp. infections: Update of systematic reviews and meta-analyses
Abstract
Introduction: Reactive arthritis (REA) and Guillain-Barré syndrome (GBS) are postinfectious complications of Campylobacter enteritis (CE); associations with inflammatory bowel diseases and irritable bowel syndrome (IBS) are also discussed. The objective of this study was to summarize existing evidence on the probability of sequelae following confirmed CE.
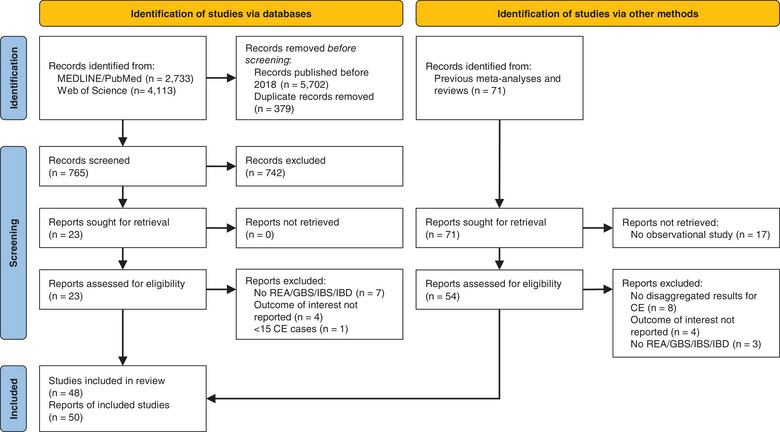
Methods: All studies included in previous reviews and meta-analyses on this topic were retrieved and assessed for eligibility; a systematic literature search was conducted to collect more recent reports. For each sequela, random effects meta-analyses were performed; the risk of bias and the quality of evidence were evaluated.
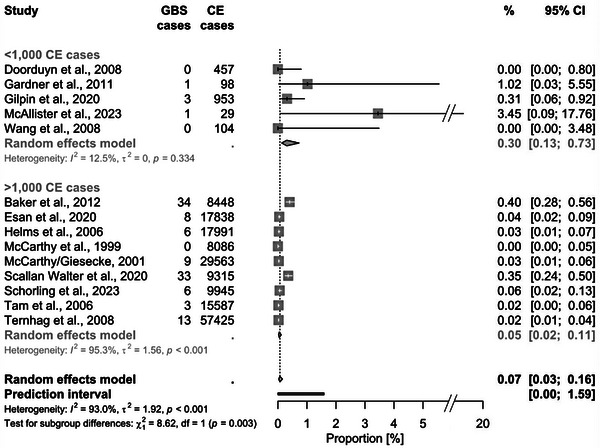
Results: In total, 50 reports of observational studies were included; between 110,765 and 175,839 CE cases were considered for each sequela. The pooled proportion of CE cases that developed a sequela was 1.72% (95% CI 0.81-3.61; prediction interval [PI]: 0.03-47.65) for REA, 0.07% (0.03-0.16; PI: 0.003-1.59) for GBS, 0.22% (0.06-0.73; PI: 0.002-20.69) for Crohn's disease (CD), 0.35% (0.11-1.15; PI: 0.003-28.16) for ulcerative colitis (UC), and 4.48% (1.92-10.08; PI: 0.09-70.62) for IBS. The high between-study heterogeneity could partially be explained by study size and design, the method of assessing sequelae, and the period between CE and sequelae onset. The quality of evidence was rated as moderate for GBS and UC, and low for REA, CD, and IBS.
Conclusion: Updated estimates of the probability to develop sequelae after CE are provided, for CD and UC for the first time. However, uncertainty regarding the true probabilities remains, which is reflected in the broad PIs.
Keywords: Campylobacter infections; Guillain–Barré syndrome; arthritis, reactive; inflammatory bowel diseases; irritable bowel syndrome; meta‐analysis.
© 2023 The Authors. Public Health Challenges published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have declared that no conflicts of interest exist.
Figures



Similar articles
-
Health care utilizations and costs of Campylobacter enteritis in Germany: A claims data analysis.PLoS One. 2023 Apr 5;18(4):e0283865. doi: 10.1371/journal.pone.0283865. eCollection 2023. PLoS One. 2023. PMID: 37018288 Free PMC article.
-
Comparative characteristics of fatigue in irritable bowel syndrome and inflammatory bowel disease: A systematic review and meta-analysis.J Psychosom Res. 2024 Feb;177:111589. doi: 10.1016/j.jpsychores.2024.111589. Epub 2024 Jan 6. J Psychosom Res. 2024. PMID: 38199049
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Systematic review with meta-analyses: does the pathogen matter in post-infectious irritable bowel syndrome?Scand J Gastroenterol. 2019 May;54(5):546-562. doi: 10.1080/00365521.2019.1607897. Epub 2019 May 21. Scand J Gastroenterol. 2019. PMID: 31112663
-
Incidence, risk factors, and health service burden of sequelae of campylobacter and non-typhoidal salmonella infections in England, 2000-2015: A retrospective cohort study using linked electronic health records.J Infect. 2020 Aug;81(2):221-230. doi: 10.1016/j.jinf.2020.05.027. Epub 2020 May 21. J Infect. 2020. PMID: 32445725
Cited by
-
Growth rates and metabolic traits differ by diarrhoeal manifestation in Campylobacter jejuni strains.J Med Microbiol. 2025 Aug;74(8):002053. doi: 10.1099/jmm.0.002053. J Med Microbiol. 2025. PMID: 40880249 Free PMC article.
-
The disease and economic burden of notified and underestimated Campylobacter enteritis cases and associated sequelae in Germany.PLoS One. 2025 Sep 4;20(9):e0331298. doi: 10.1371/journal.pone.0331298. eCollection 2025. PLoS One. 2025. PMID: 40906672 Free PMC article.
References
-
- O'Brien SJ. The consequences of Campylobacter infection. Curr Opin Gastroenterol. 2017;33:14‐20. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous