

Real-World Outcomes of Molecular Tumor Board Treatment Recommendations
- PMID: 40499091
- PMCID: PMC12175791
- DOI: 10.1200/PO-24-00387
Real-World Outcomes of Molecular Tumor Board Treatment Recommendations
Abstract
Purpose: The Molecular Tumor Board (MTB) is an important tool for the selection of molecularly targeted agents (MTAs), but its clinical utility is unconfirmed in real-world practice.
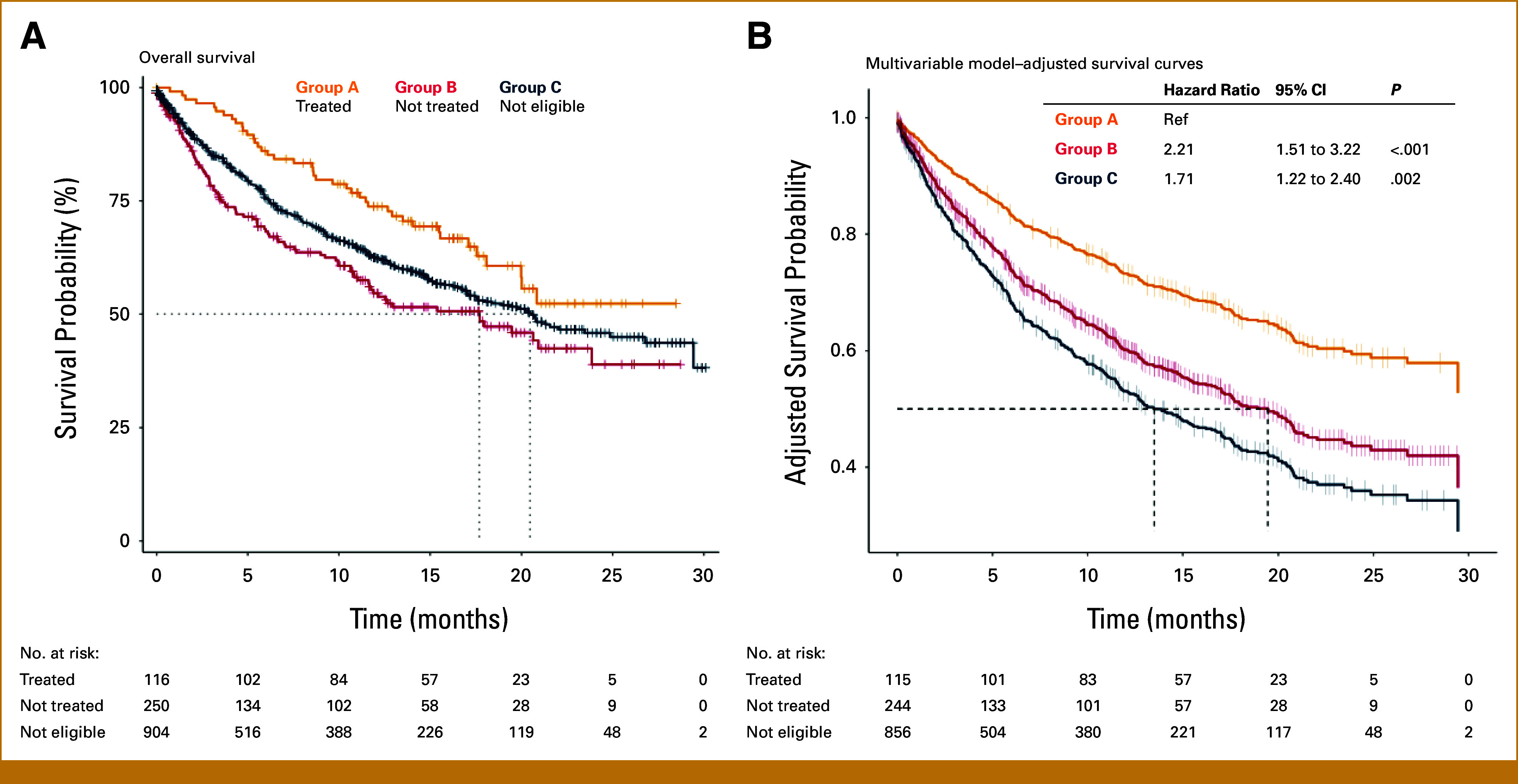
Materials and methods: We explored the clinical relevance of MTAs in patients discussed by the MTB of the National Cancer Institute of Milan. Patients were stratified into eligible (ie, at least one actionable molecular alteration identified) and treated with MTA (group A), eligible but not treated (group B), or not eligible (group C). Cases for whom a European Society for Medical Oncology Scale for Clinical Actionability of Molecular Targets IA tier target was identified were excluded from this analysis and managed as per clinical practice. The study end points were overall survival (OS), progression-free survival (PFS), and PFSratio, defined as PFS on MTA/PFS on the last previous treatment in group A.
Results: As of November 2022, 1,813 cases were discussed, of which 458 (25.2%) were potentially eligible to MTA and 117 (6.4%) started treatment. The median PFS on MTA was 12.0 months and the median PFSratio in patients receiving MTA as >1 line of treatment was 2.71, with a benefit rate of 64%. OS was significantly longer in group A than in B and C metastatic patients (adjusted hazard ratio, 2.21 and 1.71 in group B and C, respectively; P < .001).
Conclusion: Efforts should be pursued to offer MTB-driven therapies, as eligible patients who did not receive MTA showed a significantly poorer prognosis.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures


References
-
- Bedard PL, Hyman DM, Davids MS, et al. : Small molecules, big impact: 20 years of targeted therapy in oncology. Lancet 395:1078-1088, 2020 - PubMed
-
- Mosele F, Remon J, Mateo J, et al. : Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO precision medicine working group. Ann Oncol 31:1491-1505, 2020 - PubMed
-
- Mosele MF, Westphalen CB, Stenzinger A, et al. : Recommendations for the use of next-generation sequencing (NGS) for patients with advanced cancer in 2024: A report from the ESMO precision medicine working group. Ann Oncol 35:588-606, 2024 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
