

A rare case report of first-trimester intestinal obstruction masquerading as ectopic pregnancy: Insights from a low-resource setting
- PMID: 40499449
- PMCID: PMC12179728
- DOI: 10.1016/j.ijscr.2025.111484
A rare case report of first-trimester intestinal obstruction masquerading as ectopic pregnancy: Insights from a low-resource setting
Abstract
Introduction and importance: Intestinal obstruction is a rare but serious condition in pregnancy, posing significant risks to both maternal and fetal health. Its diagnosis and management are particularly challenging due to non-specific symptoms, limitations in radiological assessment during pregnancy, and the potential for surgical complications. The differentiation between obstetric and non-obstetric causes of an acute abdomen also poses a diagnostic challenge. To the best of our knowledge, this study reports one of the rarest cases of intestinal obstruction in the first trimester of pregnancy. The case was initially mistaken for an ectopic pregnancy. The condition was successfully managed surgically without the need for pregnancy termination.
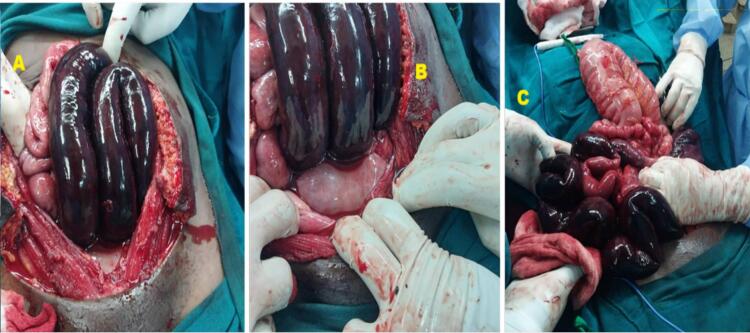
Case presentation: A 34-year-old G3P2L2 woman from Northern Tanzania presented at 12 weeks gestation with sudden-onset abdominal pain. Initial radiological findings suggested a ruptured ectopic pregnancy with extensive hemoperitoneum. The patient was taken for an emergency laparotomy where an intrauterine pregnancy was identified as well as gangrenous small bowel and sigmoid colon due to a 360-degree mesenteric rotation. Surgical intervention included bowel resection, decompression, and anastomosis of the remaining segments. The mesenteric defects were closed, and the patient had an uneventful postoperative recovery, being discharged in stable condition for conservative management.
Clinical discussion: This case report highlights the rarity of intestinal obstruction during pregnancy and the diagnostic challenges it presents. Our case is particularly unique due to the absence of previous abdominal surgery and presentation so early in gestation. There exists significant diagnostic uncertainty and resulting delays in treatment have the potential to increase the risk of maternal and fetal morbidity, especially in resource poor settings.
Conclusion: Intestinal obstruction during pregnancy is an uncommon but serious condition associated with significant maternal and fetal morbidity. Its diagnosis can be challenging, as symptoms may mimic common obstetric complications, leading to potential delays in recognition and treatment. Effective management requires a multidisciplinary approach and timely clinical decision-making to optimize outcomes for both the mother and fetus.
Keywords: Ectopic pregnancy; Gangrenous small bowel; Intestinal obstruction; Pregnancy; Sigmoid colon.
Copyright © 2025 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement All authors have declared that no competing interests exist.
Figures

References
-
- Augustin G., Majerovic M. Non-obstetrical acute abdomen during pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. Mar 1 2007;131(1):4–12. - PubMed
-
- Tan E.K., Tan E.L. Alterations in physiology and anatomy during pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. Dec 1 2013;27(6):791–802. - PubMed
-
- Angelini D.J. Obstetric triage revisited: update on non-obstetric surgical conditions in pregnancy. J. Midwifery Womens Health. Mar 1 2003;48(2):111–118. - PubMed
-
- Andersson R.E., Lambe M. Incidence of appendicitis during pregnancy. Int. J. Epidemiol. Dec 1 2001;30(6):1281–1285. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
