

Understanding acute kidney injury in cirrhosis: Current perspective
- PMID: 40501465
- PMCID: PMC12149908
- DOI: 10.4254/wjh.v17.i5.104724
Understanding acute kidney injury in cirrhosis: Current perspective
Abstract
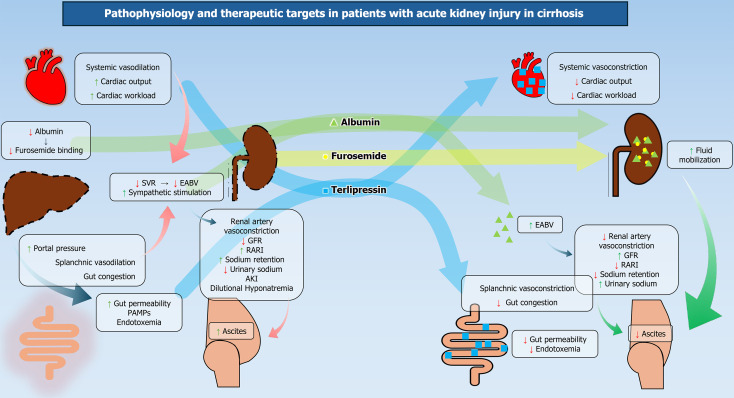
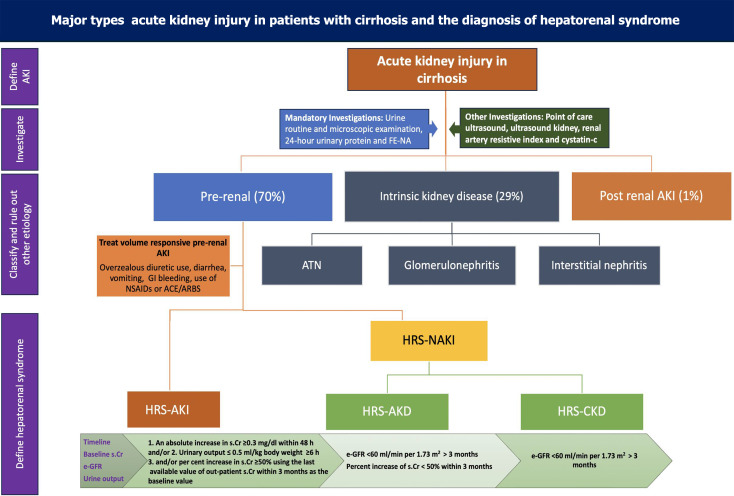
Acute kidney injury (AKI) is present in 30%-40% of hospitalized patients with cirrhosis. Its incidence is higher in patients with severe alcoholic hepatitis, spontaneous bacterial peritonitis, and acute-on-chronic-liver failure (ACLF). Kidney injury is an important landmark event in the natural history of cirrhosis as it is associated with higher mortality. Overwhelming systemic vasodilation, cardiac dysfunction, hypoperfusion, endotoxemia, and direct nephrotoxicity predispose patients with cirrhosis to kidney injury. Infection is present in 25% of patients with decompensated cirrhosis and 35%-40% of patients with ACLF. Advanced cirrhosis with portal hypertension leads to a sluggish portal flow, leading to increased gut congestion, altered gut permeability and bacterial translocations. They drive infection and endotoxemia in such patients. Pathogen-associated molecular patterns activate inflammatory cascades, which leads to further deterioration in hemodynamics and reduced glomerular filtration rate. Infections and pro-inflammatory cytokines like interleukin 6 (IL-6), IL-1, and tumor necrosis factor alpha may directly cause kidney parenchymal injury. The combined effect of dysfunctional albumin and systemic and splanchnic vasodilatation leads to low effective blood volume, activating the renin-angiotensin-aldosterone system. This causes renal vasoconstriction, water retention, and ascites, which progresses to hepatorenal physiology and AKI development. Vasoconstriction and volume expansion effectively improve arterial blood volume and systemic hemodynamics, thereby improving renal blood flow. It is of paramount importance to predict, detect, and treat AKI in its early state, as progressive renal dysfunction is invariably associated with higher mortality in patients with decompensated cirrhosis and ACLF. This comprehensive review will focus on the recent evolving concepts of the pathophysiology, diagnosis, and management of AKI in patients with cirrhosis.
Keywords: Acute kidney injury; Acute-on-chronic liver failure; Ascites; Cirrhosis; Hepatorenal syndrome.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
References
-
- Charlton MR, Wall WJ, Ojo AO, Ginès P, Textor S, Shihab FS, Marotta P, Cantarovich M, Eason JD, Wiesner RH, Ramsay MA, Garcia-Valdecasas JC, Neuberger JM, Feng S, Davis CL, Gonwa TA International Liver Transplantation Society Expert Panel. Report of the first international liver transplantation society expert panel consensus conference on renal insufficiency in liver transplantation. Liver Transpl. 2009;15:S1–34. - PubMed
-
- Trebicka J, Amoros A, Pitarch C, Titos E, Alcaraz-Quiles J, Schierwagen R, Deulofeu C, Fernandez-Gomez J, Piano S, Caraceni P, Oettl K, Sola E, Laleman W, McNaughtan J, Mookerjee RP, Coenraad MJ, Welzel T, Steib C, Garcia R, Gustot T, Rodriguez Gandia MA, Bañares R, Albillos A, Zeuzem S, Vargas V, Saliba F, Nevens F, Alessandria C, de Gottardi A, Zoller H, Ginès P, Sauerbruch T, Gerbes A, Stauber RE, Bernardi M, Angeli P, Pavesi M, Moreau R, Clària J, Jalan R, Arroyo V. Addressing Profiles of Systemic Inflammation Across the Different Clinical Phenotypes of Acutely Decompensated Cirrhosis. Front Immunol. 2019;10:476. - PMC - PubMed
-
- Albillos A, Martin-Mateos R, Van der Merwe S, Wiest R, Jalan R, Álvarez-Mon M. Cirrhosis-associated immune dysfunction. Nat Rev Gastroenterol Hepatol. 2022;19:112–134. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
