

This is a preprint.
Spatiotemporal Single-Cell Analysis Reveals T Cell Clonal Dynamics and Phenotypic Plasticity in Human Graft-versus-Host Disease
- PMID: 40501545
- PMCID: PMC12154625
- DOI: 10.1101/2025.05.24.655962
Spatiotemporal Single-Cell Analysis Reveals T Cell Clonal Dynamics and Phenotypic Plasticity in Human Graft-versus-Host Disease
Abstract
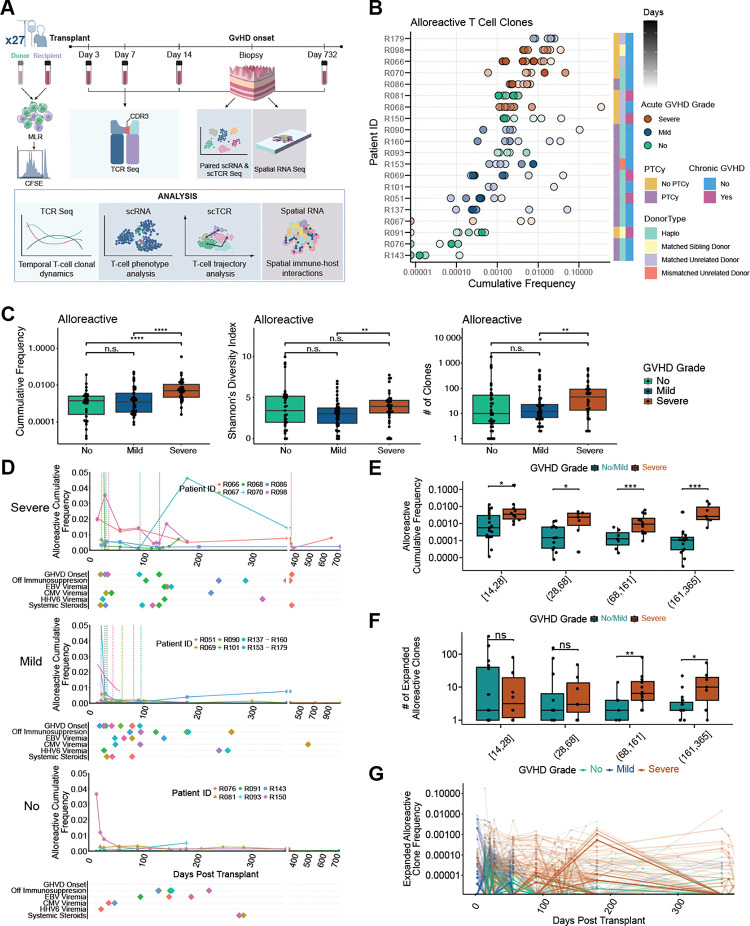
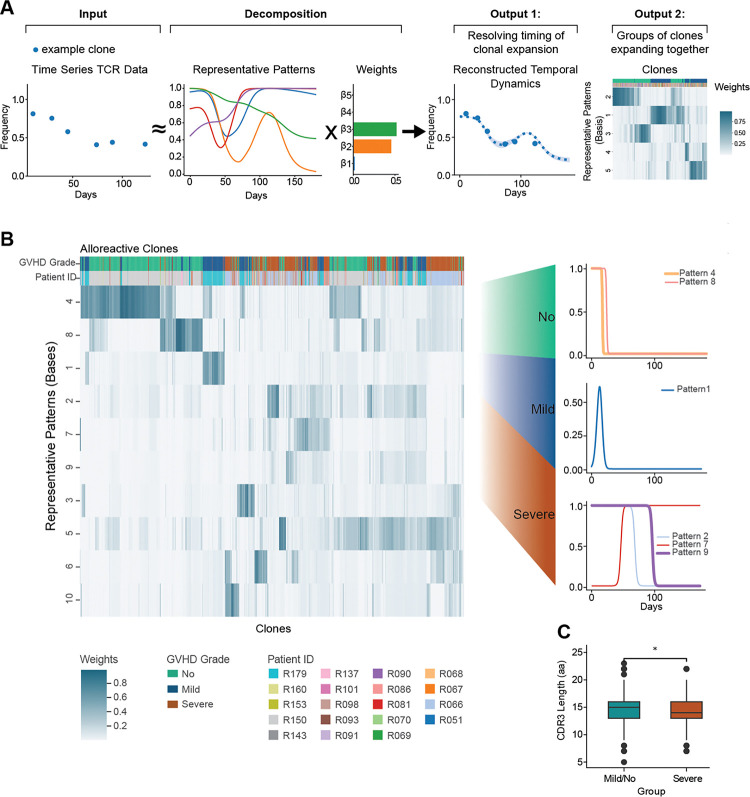
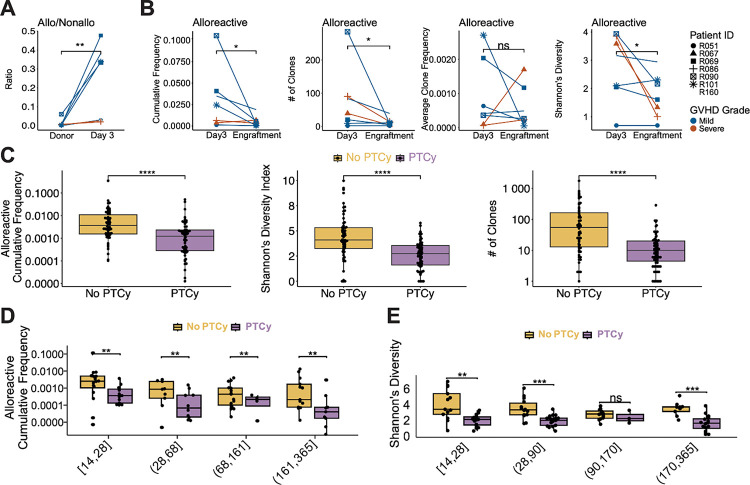
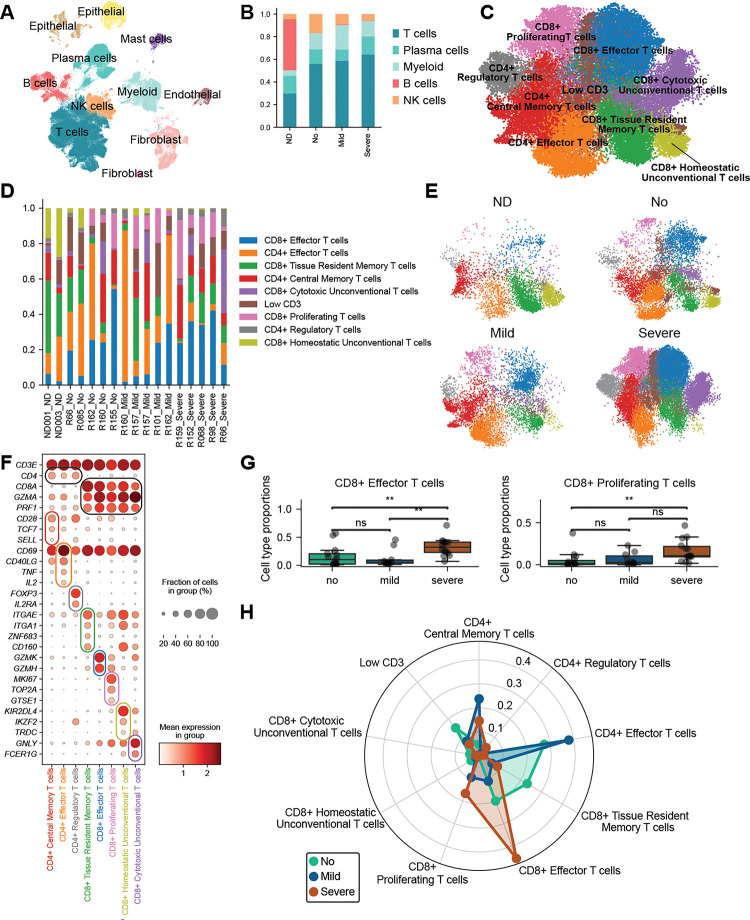
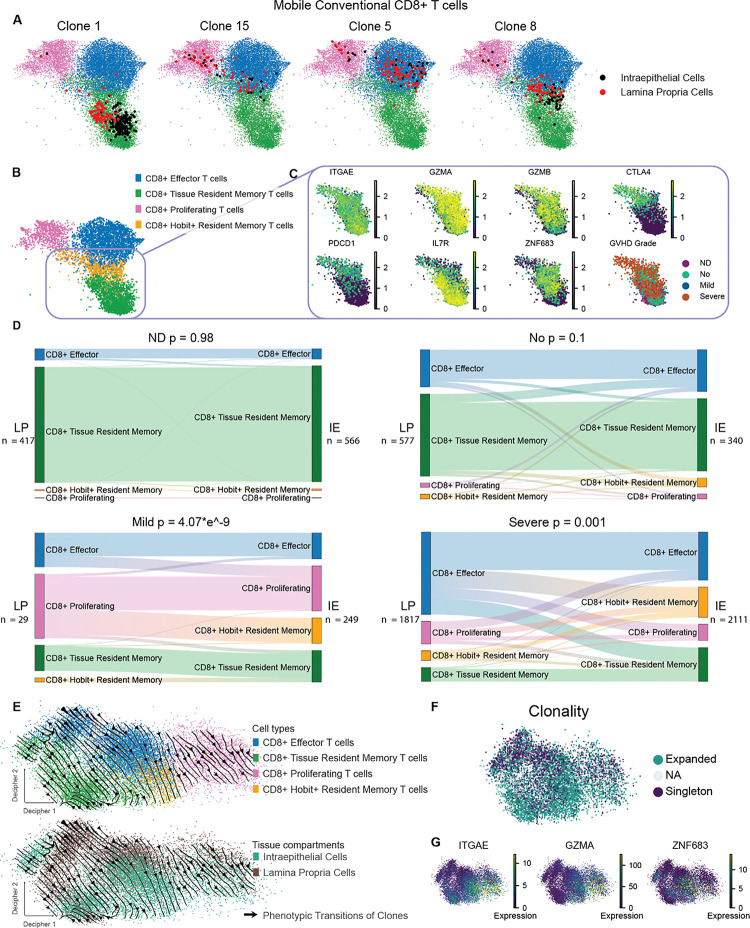
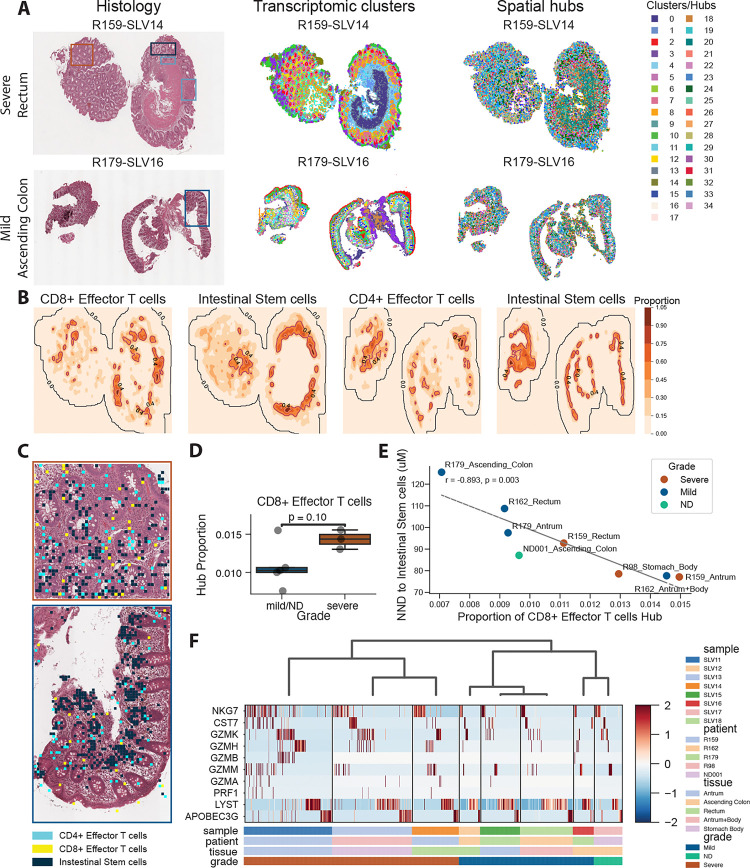
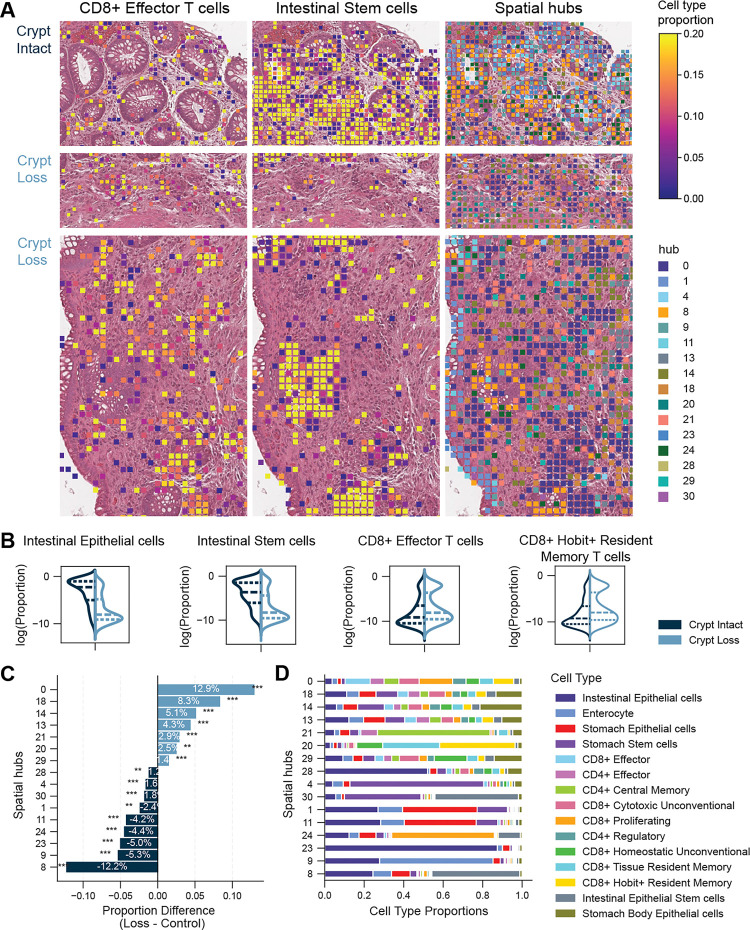
Allogeneic hematopoietic cell transplantation (alloHCT) is curative for various hematologic diseases but often leads to acute graft-versus-host disease (GVHD), a potentially life-threatening complication. We leverage GVHD as a uniquely tractable disease model to dissect complex T-cell-mediated pathology in 27 alloHCT recipients. We integrate pre-transplant identification of alloreactive T-cells with longitudinal tracking across blood and gut, using mixed lymphocyte reaction-based clonal "fingerprinting", TCR clonotyping, single-cell RNA/TCR sequencing, and spatial transcriptomics. Using DecompTCR, a novel computational tool for longitudinal TCR analysis, we uncover clonal expansion programs linked to GVHD severity and TCR features. Multi-omics profiling of gut biopsies reveals enrichment and clonal expansion of CD8+ effector and ZNF683(Hobit)+ resident memory T-cells, cytolytic remodeling of regulatory and unconventional T-cells, and localization of CD8+ effector T-cells near intestinal stem cells in crypt loss regions. This framework defines dynamic immune circuit rewiring and phenotypic plasticity with implications for biomarkers and therapies.
Keywords: Graft-versus-host disease; allogeneic hematopoietic cell transplantation; alloreactive T cells; phenotypic plasticity; probabilistic model; single-cell genomics; spatial transcriptomics; temporal dynamics.
Conflict of interest statement
Declaration of interests R.R. reports consulting or advisory role with Allogene, Bayer, Gilead Sciences, Incyte, TScan, Orca Bio, Pierre Fabre Pharmaceuticals, CareDx, Sana Biotechnology, Sail Biomedicines and Autolus, and research funding from Atara Biotherapeutics, Incyte, Sanofi, Immatics, Abbvie, Takeda, Gilead Sciences, CareDx, TScan, Cabaletta, Synthekine, BMS, J&J, Allogene, Genentech, Vittoria Therapeutics, AstraZeneca, Kinomica and Imugene.
Figures
References
-
- Zeiser R., and Blazar B.R. (2018). Acute Graft-versus-Host Disease. N. Engl. J. Med. 378, 586. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials