

Comparison of Prophylactic Transcatheter Arterial Embolization and Standard Therapy in High-Risk Non-Variceal Upper Gastrointestinal Bleeding: A Meta-Analysis
- PMID: 40503191
- PMCID: PMC12151128
- DOI: 10.14740/gr2041
Comparison of Prophylactic Transcatheter Arterial Embolization and Standard Therapy in High-Risk Non-Variceal Upper Gastrointestinal Bleeding: A Meta-Analysis
Abstract
Background: Rebleeding is a major challenge and a serious complication of non-variceal upper gastrointestinal bleeding (NVUGIB). Prophylactic transcatheter arterial embolization (P-TAE) has emerged as a potential management strategy for high-risk cases. This study aimed to evaluate the efficacy and safety of P-TAE compared with no embolization (NE) in the absence of angiographic evidence of bleeding or therapeutic arterial embolization (TAE).
Methods: The study systematically searched Medline and Embase databases from inception until November 15, 2024. The primary outcome was the overall rebleeding rate, while secondary outcomes included mortality, need for additional interventions, transfusion requirements, hospital/intensive care unit (ICU) stay, and procedure-related adverse events.
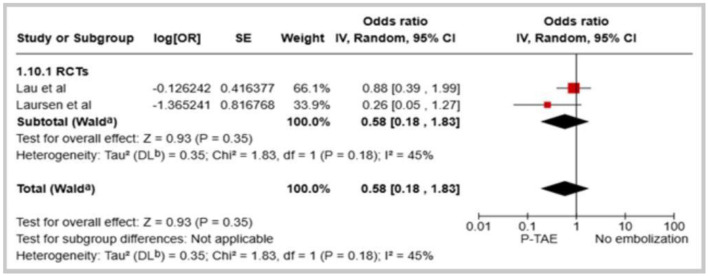
Results: The meta-analysis included 10 studies with a total population of 1,253 patients. Compared to NE, the pooled data indicated that P-TAE was not associated with significantly reduced rates of rebleeding (odds ratio (OR): 0.69, 95% confidence interval (CI): 0.39 - 1.22, P = 0.20) or all-cause mortality (OR: 0.70, 95% CI: 0.40 - 1.23). Although P-TAE trended towards lower rates of repeat interventions, blood transfusions, and shorter hospital stays, these differences were not statistically significant. Conversely, P-TAE and TAE had similar rates of rebleeding (OR: 1.08, 95% CI: 0.70 - 1.68, P = 0.05) and all-cause mortality (OR: 0.72, 95% CI: 0.34 - 1.51, P = 0.39). The analysis found no significant differences in adverse events or the need for repeat procedures between the two embolization approaches.
Conclusion: This review suggests that P-TAE may not significantly reduce rebleeding or mortality compared with standard therapy for high-risk NVUGIB. However, the current findings remain inconclusive, and further comprehensive research with larger sample sizes is required to conclusively substantiate these observations.
Keywords: Adverse events/complications; Endoscopic hemostasis; High-risk patients; Meta-analysis/systematic review; Mortality; Non-variceal upper gastrointestinal bleeding; Prophylactic transcatheter arterial embolization; Rebleeding.
Copyright 2025 Authors.
Conflict of interest statement
The author reported no conflict of interest relevant to this work.
Figures





Similar articles
-
Transcatheter arterial embolization versus surgery for refractory non-variceal upper gastrointestinal bleeding: a meta-analysis.World J Emerg Surg. 2019 Feb 1;14:3. doi: 10.1186/s13017-019-0223-8. eCollection 2019. World J Emerg Surg. 2019. PMID: 30733822 Free PMC article.
-
Prophylactic transcatheter arterial embolization reduces rebleeding in non-variceal upper gastrointestinal bleeding: A meta-analysis.World J Gastroenterol. 2021 Oct 28;27(40):6985-6999. doi: 10.3748/wjg.v27.i40.6985. World J Gastroenterol. 2021. PMID: 34790019 Free PMC article.
-
Transcatheter arterial embolization for endoscopically unmanageable non-variceal upper gastrointestinal bleeding.Scand J Gastroenterol. 2015 Jul;50(7):809-15. doi: 10.3109/00365521.2014.990503. Epub 2015 Mar 2. Scand J Gastroenterol. 2015. PMID: 25732964
-
Endoscopic hemostasis followed by preventive transarterial embolization in high-risk patients with bleeding peptic ulcer: 5-year experience.World J Emerg Surg. 2019 Sep 10;14:45. doi: 10.1186/s13017-019-0264-z. eCollection 2019. World J Emerg Surg. 2019. PMID: 31516544 Free PMC article.
-
Systematic Review and Meta-Analysis of Prophylactic Transarterial Embolization for High-Risk Bleeding Peptic Ulcer Disease.J Vasc Interv Radiol. 2021 Apr;32(4):576-584.e5. doi: 10.1016/j.jvir.2020.12.005. Epub 2021 Jan 29. J Vasc Interv Radiol. 2021. PMID: 33526343
References
LinkOut - more resources
Full Text Sources