

Periodontitis Accelerates Progression of Heart Failure With Preserved Ejection Fraction in Mice
- PMID: 40504059
- PMCID: PMC12399157
- DOI: 10.1016/j.jacbts.2025.03.002
Periodontitis Accelerates Progression of Heart Failure With Preserved Ejection Fraction in Mice
Abstract
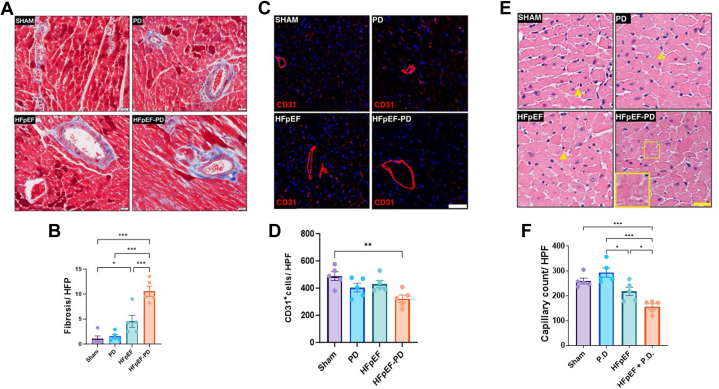
Chronic low-grade inflammation and nitric oxide (NO) depletion are important contributors to heart failure with preserved ejection fraction (HFpEF) pathophysiology. Periodontitis (PD) is a common inflammatory disease implicated in dysregulation of NO hemostasis. Epidemiological studies have shown an association between PD and increased risk of cardiovascular disease, including heart failure. However, a causative relationship between the 2 diseases has not yet been proven. In this study, we sought to investigate the direct effect of PD induction on HFpEF progression in a mouse model. Induction of PD in HFpEF mice resulted in significant oral microbial dysbiosis, accelerated progression of diastolic dysfunction by echocardiography, and increased myocardial inflammation and fibrosis. These deleterious effects seen with PD were shown to be mediated by increased systemic blood pressure, increased systemic inflammation, and NO depletion. Our study provides evidence of potential mechanistic links between PD and HFpEF progression and suggests PD as a new therapeutic target for HFpEF.
Keywords: endothelial dysfunction; heart failure with preserved ejection fraction; inflammation; nitric oxide; oral microbiome; periodontitis.
Copyright © 2025. Published by Elsevier Inc.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported in part by a grant from the Israel science foundation (ISF) (to Dr Asleh). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures







References
-
- Borlaug B.A., Sharma K., Shah S.J., Ho J.E. Heart failure with preserved ejection fraction: JACC scientific statement. J Am Coll Cardiol. 2023;81:1810–1834. - PubMed
-
- Dunlay S.M., Roger V.L., Redfield M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017;14:591–602. - PubMed
-
- Shah K.S., Xu H., Matsouaka R.A., et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. 2017;70:2476–2486. - PubMed
LinkOut - more resources
Full Text Sources
