

Azacitidine, Venetoclax, and Revumenib for Newly Diagnosed NPM1-Mutated or KMT2A-Rearranged AML
- PMID: 40504618
- PMCID: PMC12316144
- DOI: 10.1200/JCO-25-00914
Azacitidine, Venetoclax, and Revumenib for Newly Diagnosed NPM1-Mutated or KMT2A-Rearranged AML
Abstract
Purpose: Azacitidine and venetoclax is a standard frontline treatment regimen for newly diagnosed older adults with AML; however, long-term outcomes remain poor. Revumenib is an oral menin inhibitor with clinical activity in AML patients with nucleophosmin-1 mutation (NPM1m) or lysine methyltransferase 2A rearrangements (KMT2Ar).
Methods: We conducted a phase I dose-escalation and expansion study of azacitidine, venetoclax, and revumenib at two dose levels (113 mg or 163 mg orally every 12 hours in combination with strong cytochrome P450 inhibitor azoles) in patients aged 60 years and older newly diagnosed with AML with NPM1m or KMT2Ar (ClinicalTrials.gov identifier: NCT03013998).
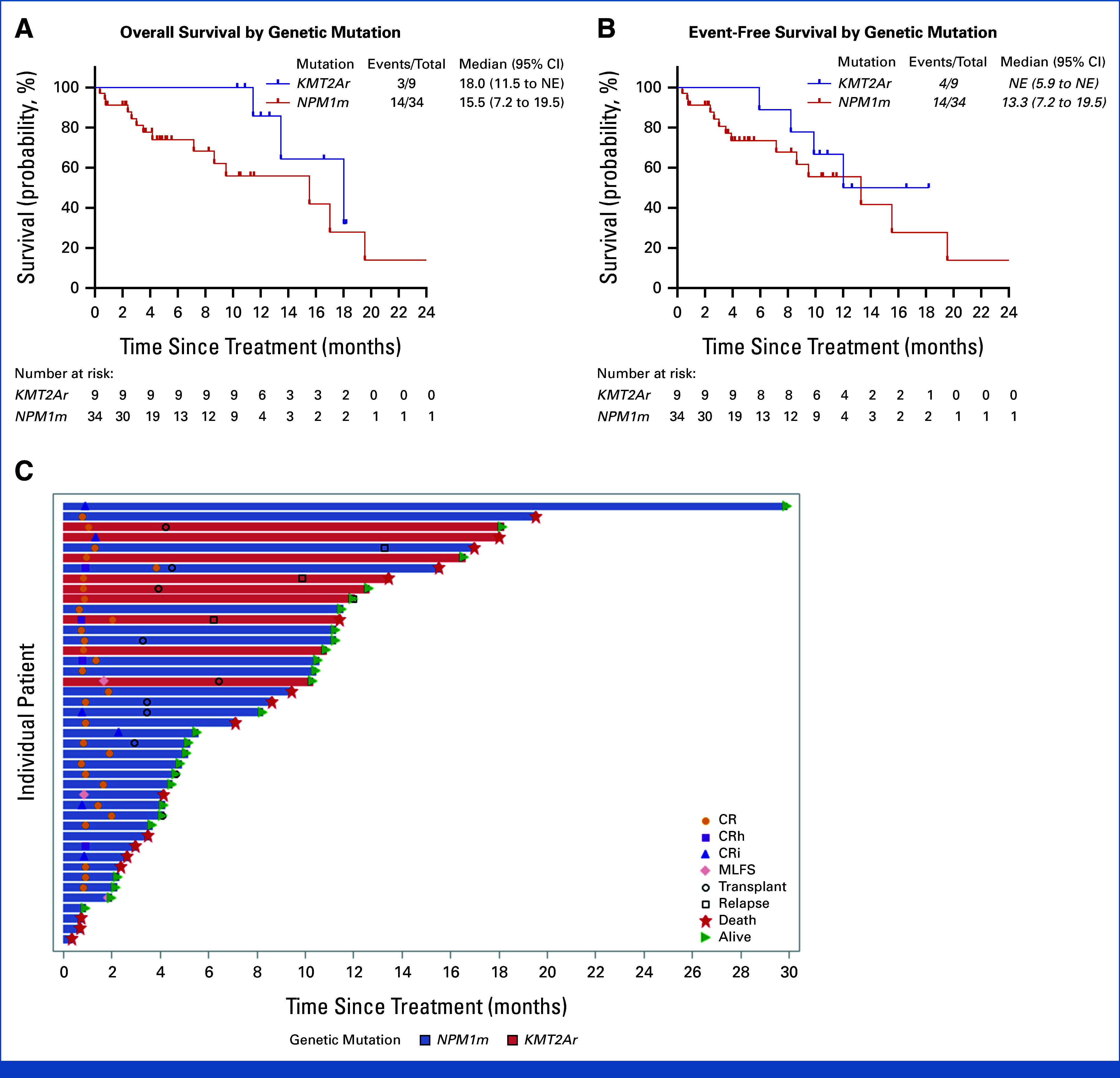
Results: Overall, 43 patients were enrolled and treated. There was no maximal tolerated dose identified. Differentiation syndrome was present in eight (19%) patients and QTc Fridericia prolongation was present in 19 (44%) patients, and neither required permanent discontinuation of revumenib. The overall response rate with an intention-to-treat population was 88.4% (95% CI, 74.9 to 96.1; NPM1m: 85.3%; KMT2Ar: 100%), the rate of composite complete remission (complete remission [CR] + CR with partial or incomplete hematologic recovery) was 81.4% (95% CI, 66.6 to 91.6; NPM1m: 79.4%; KMT2Ar: 88.9%), and the rate of CR was 67.4% (95% CI, 51.5 to 80.9; NPM1m: 65%; KMT2Ar: 78%). No patient had refractory disease after 1-2 cycles of treatment. The median time to first response was 28 days, and 84% of responders achieved remission within the first cycle. All 37 patients evaluated had no evidence of measurable residual disease by a centralized flow cytometry assay.
Conclusion: In older adults newly diagnosed with NPM1m or KMT2Ar AML, the combination of azacitidine, venetoclax, and revumenib was able to be safely administered with high rates of CR and clinical activity.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures



References
-
- DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. N Engl J Med. 2020;383:617–629. - PubMed
-
- Pratz KW, Jonas BA, Pullarkat V, et al. Long-term follow-up of VIALE-A: Venetoclax and azacitidine in chemotherapy-ineligible untreated acute myeloid leukemia. Am J Hematol. 2024;99:615–624. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
