

A macrophage-predominant immunosuppressive microenvironment and therapeutic vulnerabilities in advanced salivary gland cancer
- PMID: 40506428
- PMCID: PMC12162891
- DOI: 10.1038/s41467-025-60421-0
A macrophage-predominant immunosuppressive microenvironment and therapeutic vulnerabilities in advanced salivary gland cancer
Abstract
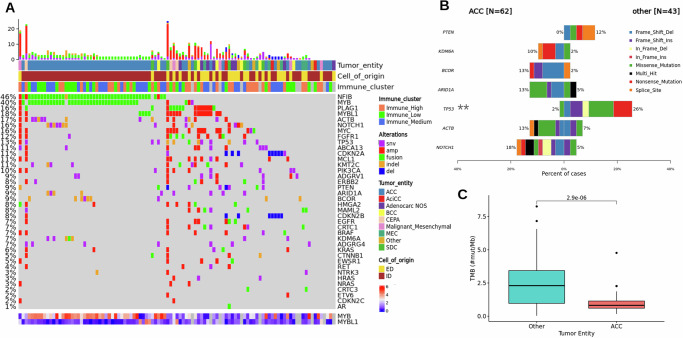
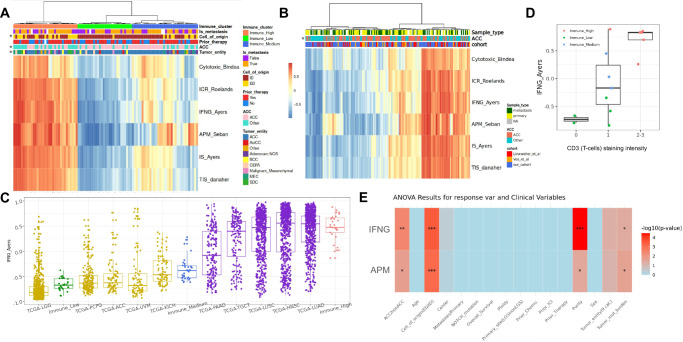
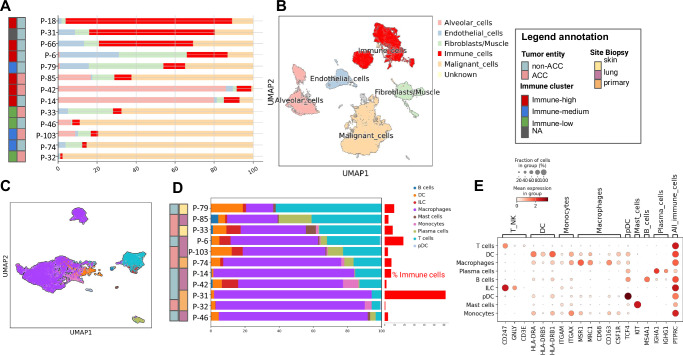
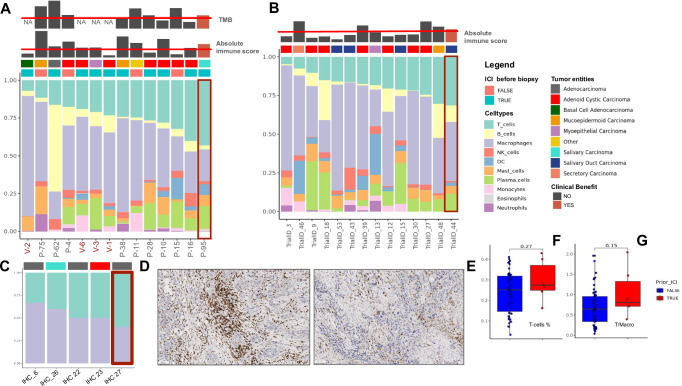
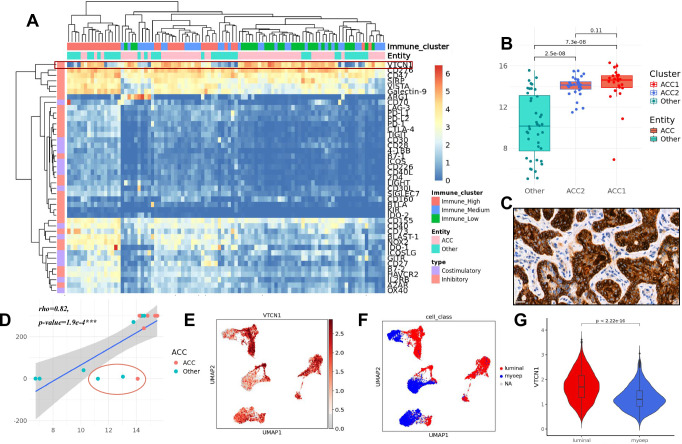
Salivary gland cancers are rare, diverse malignancies characterized by poor response to immunotherapy. The tumor immune environment in these cancers remains poorly understood. To address this, we perform an integrative analysis of the tumor immune microenvironment in a large cohort of advanced salivary gland cancer samples. Most tumors exhibit low immune activity with limited immune cell infiltration. Inflammation is linked to higher tumor mutational burden in non-adenoid cystic carcinoma histologies. Subtype specific expression of immune checkpoints is identified with prominent expression of VTCN1 in luminal-like cells within adenoid cystic carcinoma. Macrophages with immunosuppressive properties dominate the immune microenvironment across subtypes. Responses to immunotherapy are limited and associated with a higher ratio of T-cells relative to macrophages in individual cases, warranting further investigation. Here, we show an immunosuppressive environment in salivary gland cancers and identify subtype-specific immune vulnerabilities that could inform tailored therapeutic strategies.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: C.H. received honoraria, research funding and/or consulting/advisory board from Roche, Novartis, and Boehringer Ingelheim. S.F. reports consultancy fees from Illumina, DTR has received honoraria, research support, and/or travel/accommodation expenses from Bayer, Eli Lilly, Bristol-Myers Squibb, Roche, BeiGene, J&J, and Seagen. The remaining authors report no competing interests.
Figures


References
-
- Nam, S. J. et al. Risk factors and survival associated with distant metastasis in patients with carcinoma of the salivary gland. Ann. Surg. Oncol.23, 4376–4383 (2016). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
