

Complement activation profiles in patients with immune checkpoint inhibitor-associated neuromuscular immune-related adverse events
- PMID: 40506552
- PMCID: PMC12162679
- DOI: 10.1007/s00415-025-13181-2
Complement activation profiles in patients with immune checkpoint inhibitor-associated neuromuscular immune-related adverse events
Abstract
Background: Immune-related neuropathy (irNeuropathy) and myositis (irMyositis) are the most common neurologic adverse events (irAE-n) associated with immune checkpoint inhibitors. Although case reports suggest benefits of complement inhibitors, the role of complement activation in irAE-n is understudied.
Methods: In a retrospective multicenter study, we enrolled patients with irNeuropathy or irMyositis, cancer controls (CCs), and healthy controls (HCs). Serum levels of 11 complement components were measured using multiplex enzyme-linked immunosorbent assays. Associations with irAE-n severity and outcomes were assessed by Spearman's correlation. C5b-9-positive complement deposition was analyzed in muscle and nerve specimens from a subset of patients.
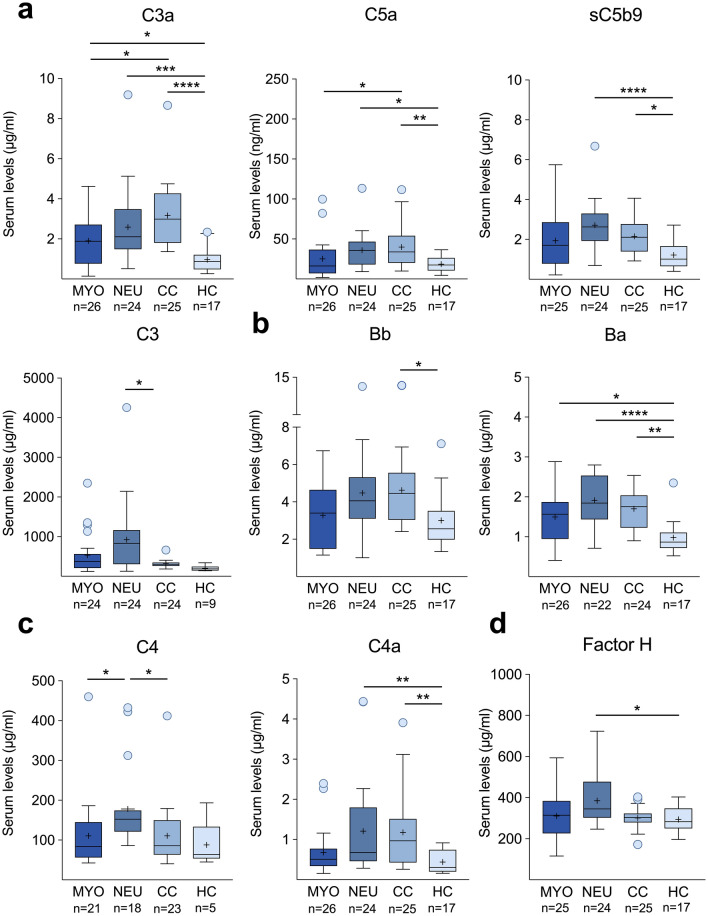
Results: Thirty-one irMyositis patients, 25 irNeuropathy patients, 25 CCs, and 17 HCs were included. Complement component levels were elevated in irNeuropathy (C3a, C5a, sC5b-9, C3, Ba, C4a), irMyositis (C3a, Ba), and CCs (C3a, C5a, sC5b-9, Bb, Ba, C4a), compared to HCs. In irMyositis, higher levels of C5a and complement regulators Factor H and I correlated with lower irAE-n severity (p = 0.02, rho = -0.45; p = < 0.01, rho = -0.56; p = < 0.001, rho = -0.67, respectively), and improved outcomes (p = 0.03, rho = -0.42; p = 0.05, rho = -0.40; p = < 0.001, rho = -0.64, respectively). Subtle C5b-9 deposition was detected in all tissue samples but showed non-specific patterns.
Discussion: Systemic complement activation is detectable in cancer patients regardless of irAE-n status, and tissue complement deposition is unspecific. Our findings suggest that complement activation is not a major driver of irAE-n, leaving the therapeutic potential of complement inhibitors uncertain.
Keywords: Complement activation; Immune checkpoint inhibitor; Immune-related adverse events; Myositis; Neuropathy; Neurotoxicity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: L. Müller-Jensen, S. Carl, J. Thomas, L. Grote-Levi, S. Nay, P. Ivanyi, I. von Wassielewski, C. Dittmayer., W. Stenzel, S. Knauss and M. Endres declare that they have no conflict of interest. N. Möhn received speaker’s honoraria from Biogen, Merck, and Novartis as well as travel grants from Biogen, Merck, and Novartis, all of which were not related to the submitted work. T. Skripuletz has received grants from the German Ministry for Education and Research (BMBF: CurePML01EN2302), the Bristol Myers Squibb Foundation for Immuno-Oncology (FA 19–010), the Claudia von Schilling Foundation for Breast Cancer Research, the Else Kröner Fresenius Foundation, the Erwin-Röver-Stiftung, Hannover Biomedical Research School (HBRS) and the VHV Foundation. He also received consulting fees and/or speaker’s honoraria by Alexion, Alnylam Pharmaceuticals, argenx, Bayer Vital, Biogen, Bristol Myers Squibb, Centogene, CSL Behring, Euroimmun, Grifols, Hexal AG, Horizon, Janssen-Cilag, Merck Serono, Novartis, Pfizer, Roche, Sanofi, Siemens, Swedish Orphan Biovitrum, Teva, and Viatris, all outside the scope of the submitted work. R. Gutzmer has received grants from Amgen, Sanofi-Regeneron, Merck Serono, Kyowa Kirin, Almirall, SUN Pharma, and Recordati. He has also received consulting fees and serves as a medical advisor for Bristol Myers Squibb, Novartis, MSD, Almirall-Hermal, Amgen, Pierre Fabre, Merck Serono, SUN, Sanofi, Immunocore, Delcath, and Kyowa Kirin. Additionally, he has received speaker’s honoraria and/or equipment from Bristol Myers Squibb, Novartis, MSD, Almirall-Hermal, Amgen, Merck Serono, SUN Pharma, Pierre Fabre, and Sanofi-Regeneron, as well as travel support from SUN Pharma and Pierre Fabre, all not related to the current work. J.D. Lünemann has received speaker fees, research support and travel support from and/or served on advisory boards for AbbVie, Alexion, Adivo, Amgen, Argenx, Biogen, CSL Behring, Janssen-Cilag, Merck, Moderna, Novartis, Roche, Sanofi, Takeda, and UCB Pharma. W. Boehmerle has received consulting fees and/or speaker’s honoraria from Osmol Therapeutics, the Charité Research Organization, Alexion, Sanofi, Bristol Myers Squibb and NOGGO e.V., all not related to the submitted work. P. Huehnchen has received grants from the German Ministry for Education and Research (BMBF) and the German Research Foundation (DFG) and was granted speaker’s honoraria by the Nord-Ostdeutsche Gesellschaft für Gynäkologische Onkologie e.V., all not related to the submitted work. Ethical approval and patient consent: The study protocol received approval from the Hannover Medical School Ethics Committee (No. 8685_BO_K2019) and the institutional review board of Charité Universitätsmedizin Berlin (EA1/099/17 and EA4/219/21). The study adhered to the principles outlined in the Declaration of Helsinki. All patients provided written informed consent to participate and publish.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
