

A Randomized, Double-Blind, Placebo-Controlled Trial of Abatacept for the Treatment of Relapsing, Nonsevere Granulomatosis With Polyangiitis
- PMID: 40506793
- PMCID: PMC12413890
- DOI: 10.1002/art.43272
A Randomized, Double-Blind, Placebo-Controlled Trial of Abatacept for the Treatment of Relapsing, Nonsevere Granulomatosis With Polyangiitis
Abstract
Objective: To compare the efficacy of abatacept to placebo for the treatment of relapsing, nonsevere granulomatosis with polyangiitis (GPA).
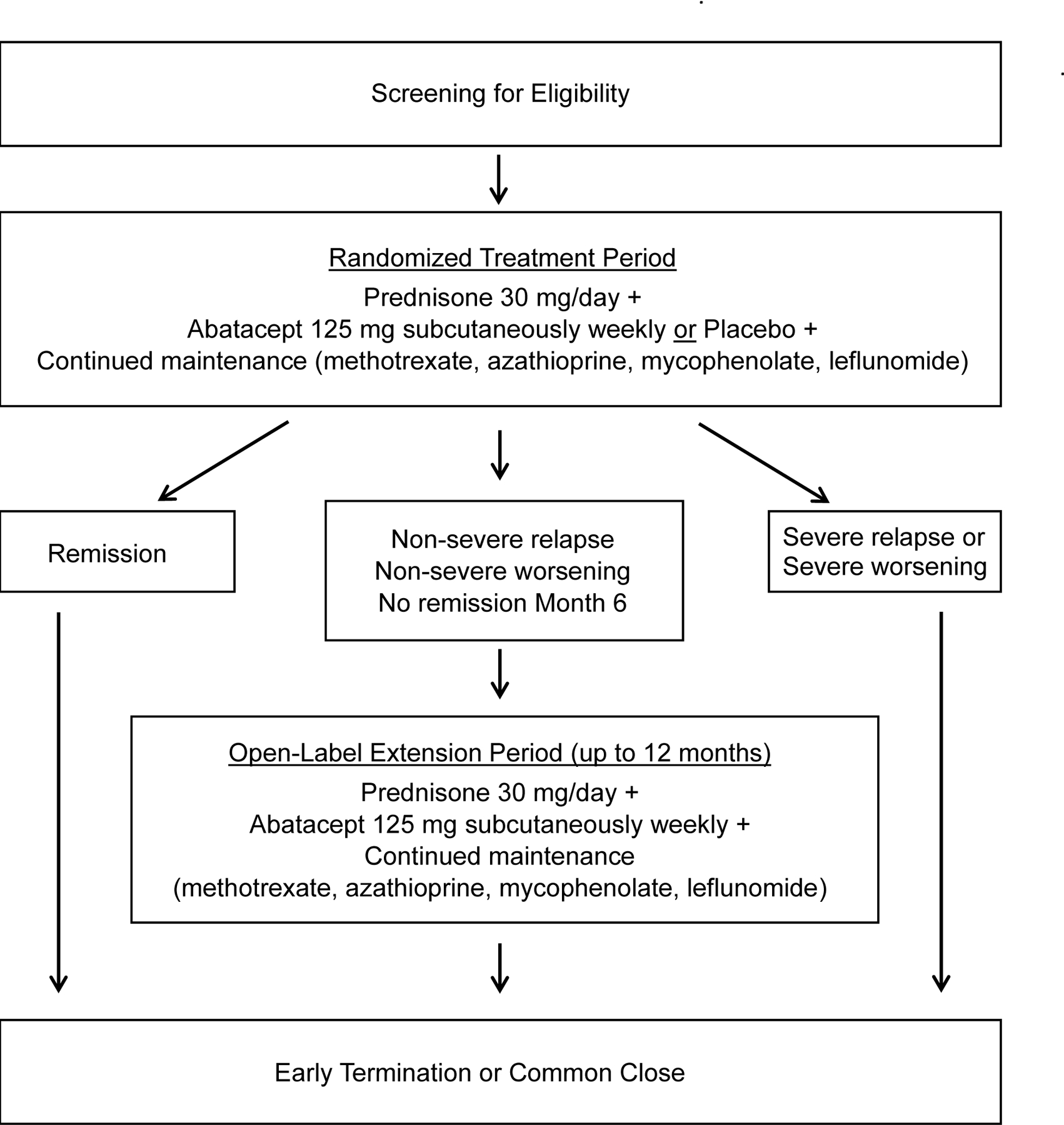
Methods: In this multicenter trial, eligible patients with relapsing, nonsevere GPA were randomized to receive abatacept 125 mg subcutaneously once a week or placebo, both together with prednisone 30 mg/day (or equivalent), tapered and discontinued at week 12. Patients already taking methotrexate, azathioprine, mycophenolate, or leflunomide continued this medication at a stable dose. Patients achieving remission remained on their randomized assignment until relapse, early termination, or the common close date 12 months after enrollment of the last patient. Those who had a nonsevere relapse, had nonsevere worsening, or were not in remission by month 6 had the option to receive open-label abatacept. The primary end point was the rate of treatment failure, defined as relapse, disease worsening, or failure to achieve a Birmingham Vasculitis Activity Score for Wegener's Granulomatosis (BVAS/WG) of 0 or 1 by six months.
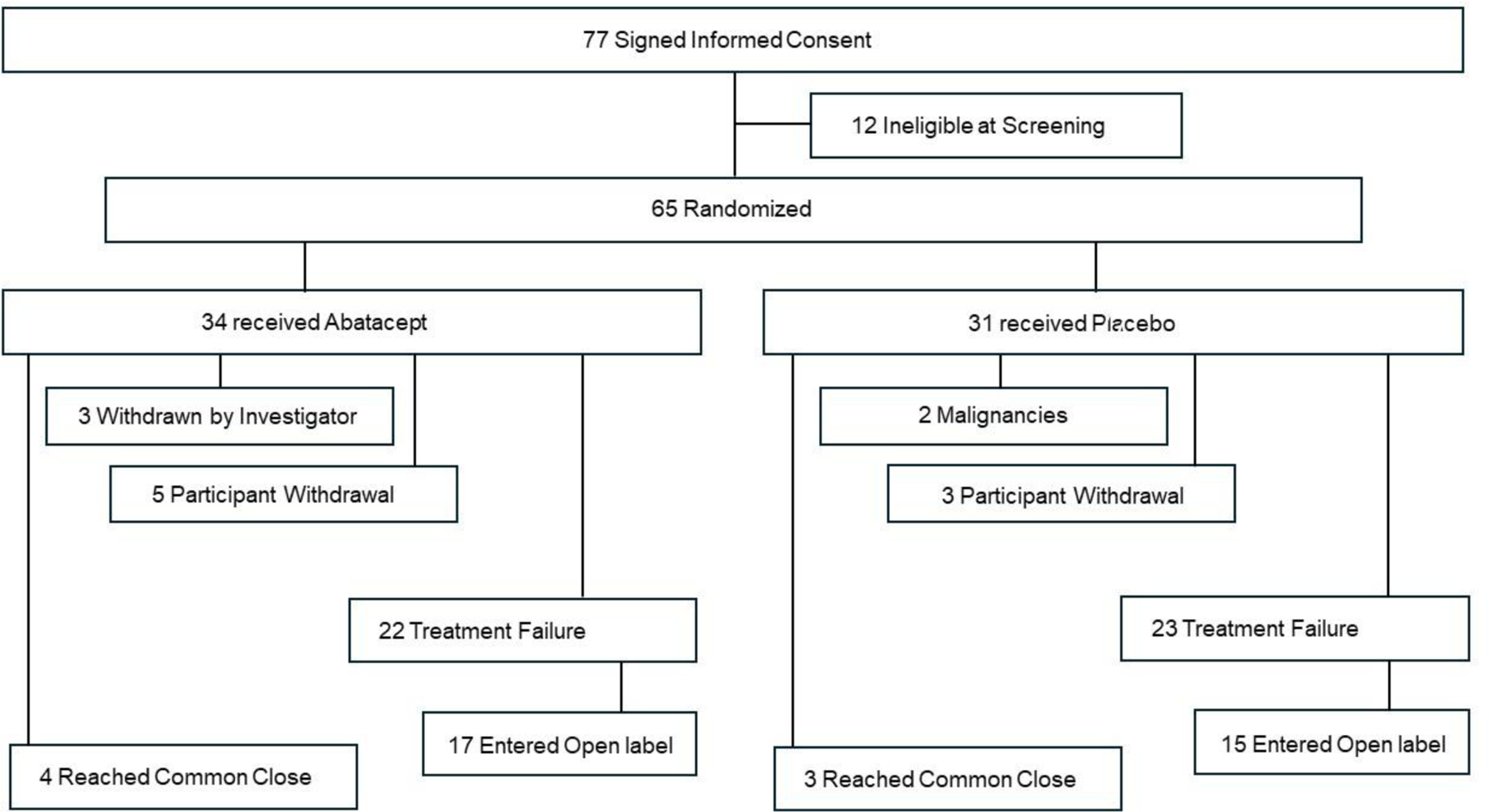
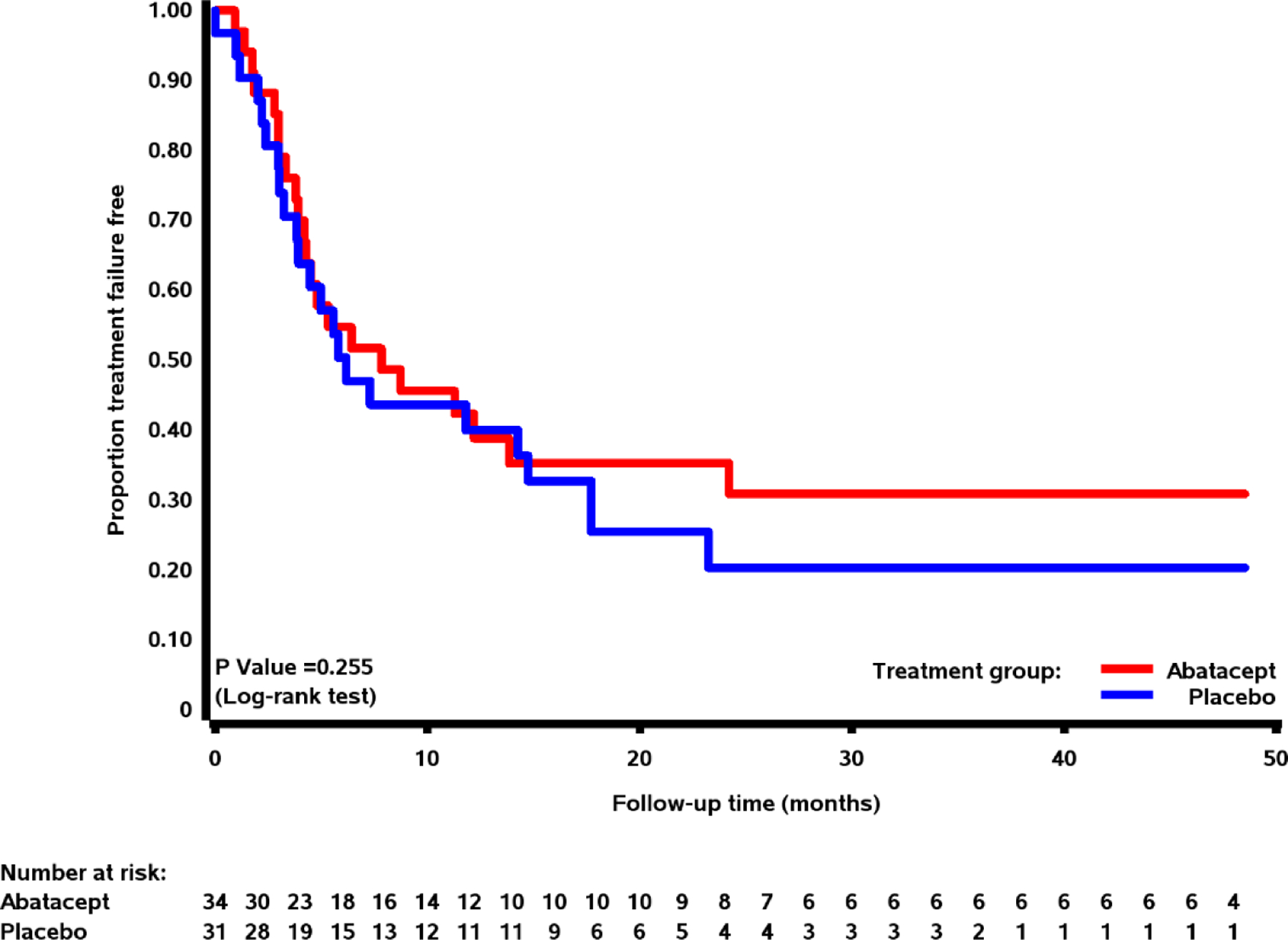
Results: Sixty-five patients were randomized; 34 received abatacept and 31 received placebo. No statistical difference in the treatment failure rate was found between those who received abatacept and those who received placebo (P = 0.853). Treatment with abatacept did not demonstrate any statistical difference from placebo in key secondary end points, including time to full remission (BVAS/WG = 0), duration of glucocorticoid-free remission, relapse severity, prevention of damage, and patient-reported quality-of-life outcomes. There was no difference in the frequency or severity of adverse events between treatment arms, including infection.
Conclusion: In patients with relapsing, nonsevere GPA, abatacept did not reduce the risk of relapse, severe worsening, or failure to achieve remission.
© 2025 The Author(s). Arthritis & Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures
References
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992;116:488–98. - PubMed
-
- Wegener’s Granulomatosis Etanercept Trial (WGET) Research Group. Etanercept plus standard therapy for Wegener’s granulomatosis. N Engl J Med 2005;352:351–61 - PubMed
-
- Stone JH; Wegener’s Granulomatosis Etanercept Trial Research Group. Limited versus severe Wegener’s granulomatosis: baseline data on patients in the Wegener’s granulomatosis etanercept trial. Arthritis Rheum 2003;48:2299–309. - PubMed
-
- Ludviksson BR, Sneller MC, Chua KS, Talar-Williams C, Langford CA, Ehrhardt RP et al. Active Wegener’s granulomatosis is associated with HLADR+CD4+ T cells exhibiting an unbalanced Th1-type T cell cytokine pattern: reversal with IL-10. J Immunol 1998;160:3602–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
