

Pelvic Pain Symptoms and Inflammation Among Adolescents and Adults with and Without Endometriosis
- PMID: 40508188
- PMCID: PMC12156163
- DOI: 10.3390/ijms26115377
Pelvic Pain Symptoms and Inflammation Among Adolescents and Adults with and Without Endometriosis
Abstract
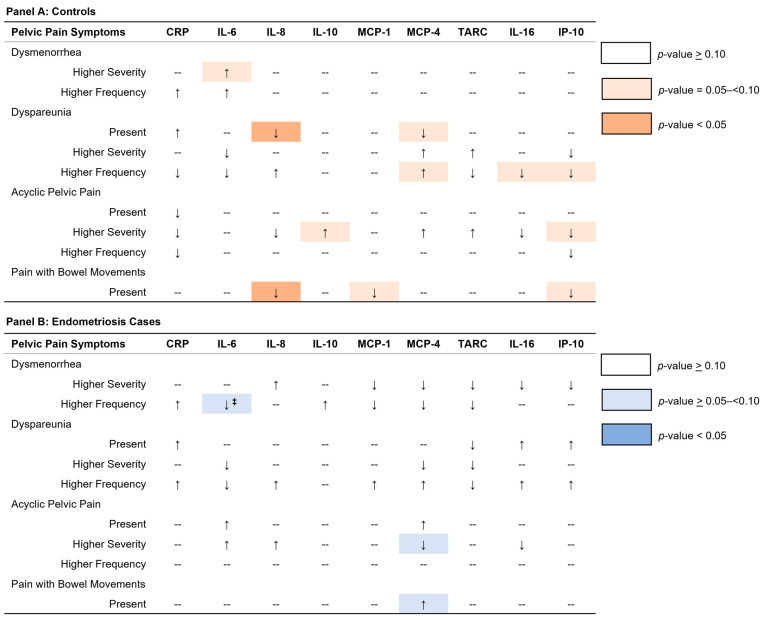
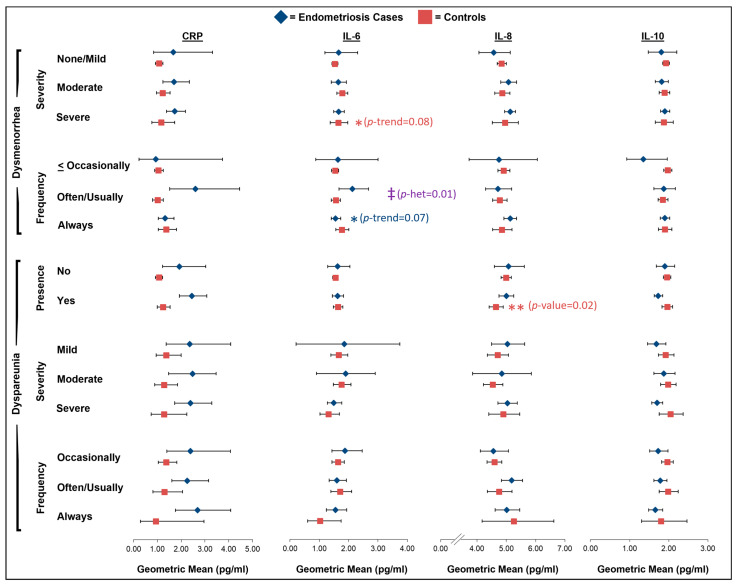
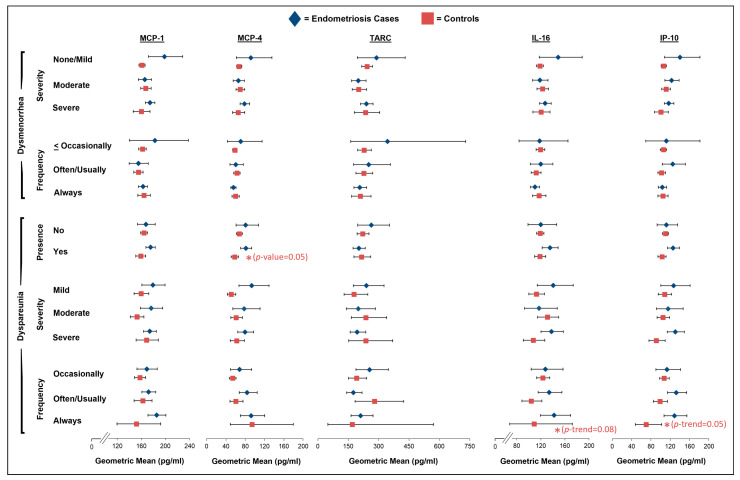
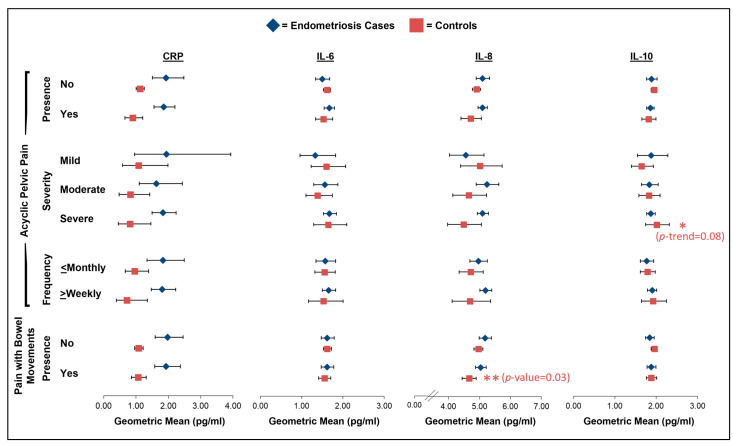
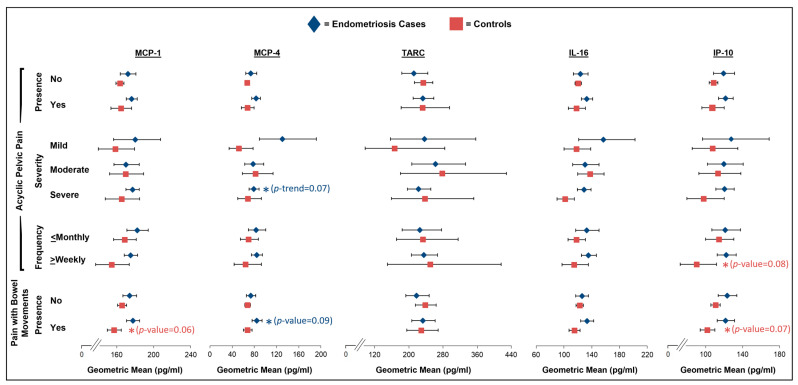
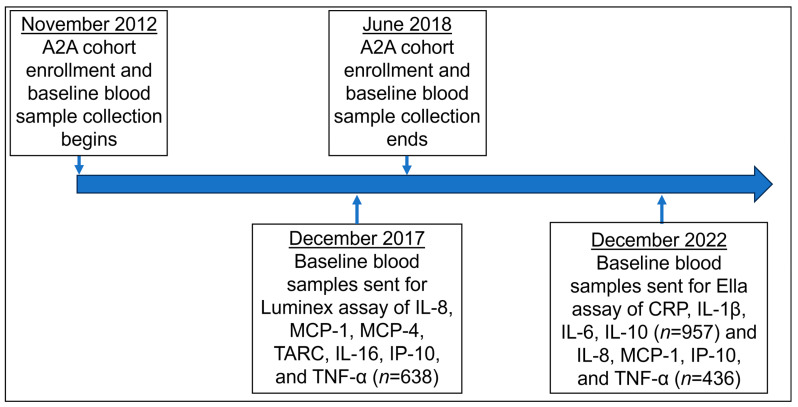
We evaluated inflammatory markers among 389 surgically confirmed endometriosis cases and 505 controls from the Women's Health Study: From Adolescence to Adulthood (A2A) cohort. Participants reported dysmenorrhea, acyclic pelvic pain, dyspareunia, and pain with bowel movements. Using multiplex assays, we measured their levels of plasma interleukin (IL)-1β, -6, -8, -10, and -16, tumor necrosis factor (TNF)-α, monocyte chemotactic protein (MCP)-1 and -4, thymus and activation-regulated chemokine (TARC), and interferon gamma-induced protein (IP)-10. For each symptom, we computed biomarker-level geometric means (GMs) with 95% confidence intervals (95% CI) using multivariate linear regression among the endometriosis cases and controls, with interactions with case/control status tested using Wald statistics. Among the controls, those with dyspareunia had lower levels of IL-8 (GMpresent = 4.64 [95% CI = 4.41-4.89] pg/mL vs. GMabsent = 4.99 [95% CI = 4.82-5.17] pg/mL; p = 0.02), and the IL-8 levels were lower for controls reporting pain with bowel movements (GMpresent = 4.66 [95% CI = 4.43-4.89] vs. GMabsent = 4.96 [95% CI = 4.82-5.11] pg/mL, p = 0.03). No significant associations between pelvic pain symptoms and inflammatory markers were observed among the endometriosis cases; however, the relationship between inflammatory marker levels and pain experience varied by analgesic use at blood draw. Dyspareunia and pain with bowel movements were associated with inflammatory markers among the controls, while the associations between pelvic pain symptoms and inflammatory markers among the endometriosis cases differed by analgesic use.
Keywords: bowel pain; chemokines; cytokines; dysmenorrhea; dyspareunia; endometriosis; inflammation; pelvic pain.
Conflict of interest statement
S.A. has served as a consultant on endometriosis and pelvic pain for Sumitomo, Bayer, Organon, and Gesynta and receives author royalties from UpToDate for expert chapters on the evaluation and management of chronic pelvic pain and endometriosis; none of these are related to this work. S.A.M. has participated in working groups for Roche, LIDEAR, and Gideon Richter, is an advisory board member for NextGen Jane, and receives grant funding from AbbVie; none of these are related to this work. K.L.T. receives grant funding from Aspira, which is unrelated to this work. All the other authors have no conflicts of interest to disclose. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Pelvic pain symptoms and endometriosis characteristics in relation to oxidative stress among adolescents and adults with and without surgically-confirmed endometriosis.F1000Res. 2024 Jan 8;13:34. doi: 10.12688/f1000research.141793.1. eCollection 2024. F1000Res. 2024. PMID: 38495219 Free PMC article.
-
Trends in pelvic pain symptoms over 2 years of follow-up among adolescents and young adults with and without endometriosis.Pain. 2023 Mar 1;164(3):613-624. doi: 10.1097/j.pain.0000000000002747. Epub 2022 Aug 9. Pain. 2023. PMID: 35947080 Free PMC article.
-
Plasma proteomic profiles of pain subtypes in adolescents and young adults with endometriosis.Hum Reprod. 2023 Aug 1;38(8):1509-1519. doi: 10.1093/humrep/dead099. Hum Reprod. 2023. PMID: 37196326 Free PMC article.
-
The effect of endometriosis on sexual function as assessed with the Female Sexual Function Index: systematic review and meta-analysis.Gynecol Endocrinol. 2020 Nov;36(11):1015-1023. doi: 10.1080/09513590.2020.1812570. Epub 2020 Sep 3. Gynecol Endocrinol. 2020. PMID: 32880200
-
Secondary dysmenorrhea and dyspareunia associated with pelvic girdle dysfunction: A case report and review of literature.J Bodyw Mov Ther. 2021 Jul;27:165-168. doi: 10.1016/j.jbmt.2021.03.013. Epub 2021 Mar 19. J Bodyw Mov Ther. 2021. PMID: 34391229 Review.
References
-
- Ghiasi M., Chang C., Shafrir A.L., Vitonis A.F., Sasamoto N., Vazquez A.I., DiVasta A.D., Upson K., Sieberg C.B., Terry K.L., et al. Subgroups of pelvic pain are differentially associated with endometriosis and inflammatory comorbidities: A latent class analysis. Pain. 2024;165:2119–2129. doi: 10.1097/j.pain.0000000000003218. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
