

Regenerative Endodontic Therapies: Harnessing Stem Cells, Scaffolds, and Growth Factors
- PMID: 40508718
- PMCID: PMC12157830
- DOI: 10.3390/polym17111475
Regenerative Endodontic Therapies: Harnessing Stem Cells, Scaffolds, and Growth Factors
Abstract
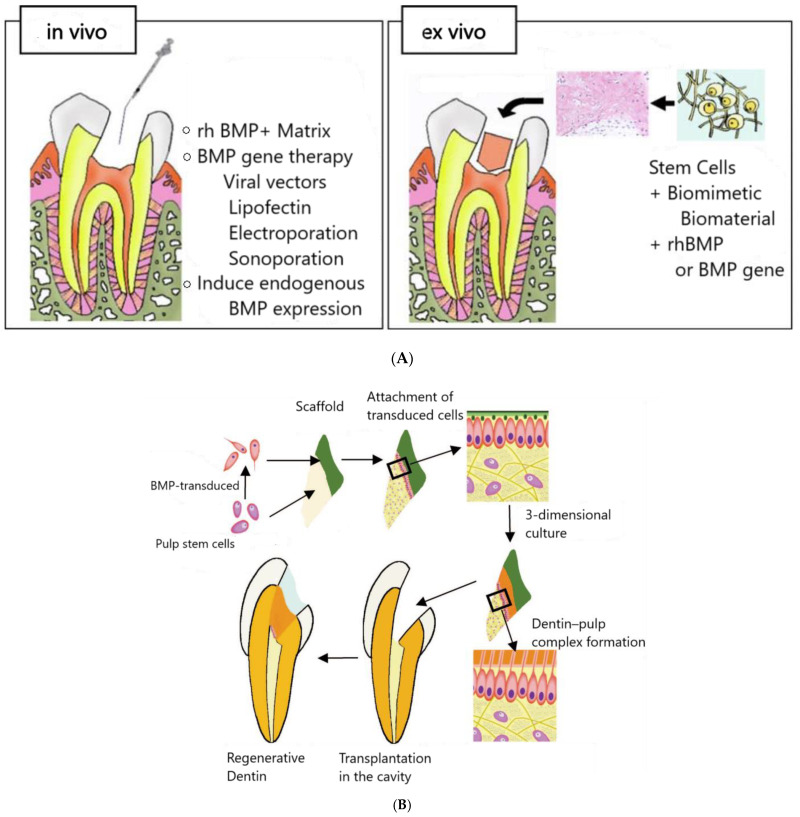
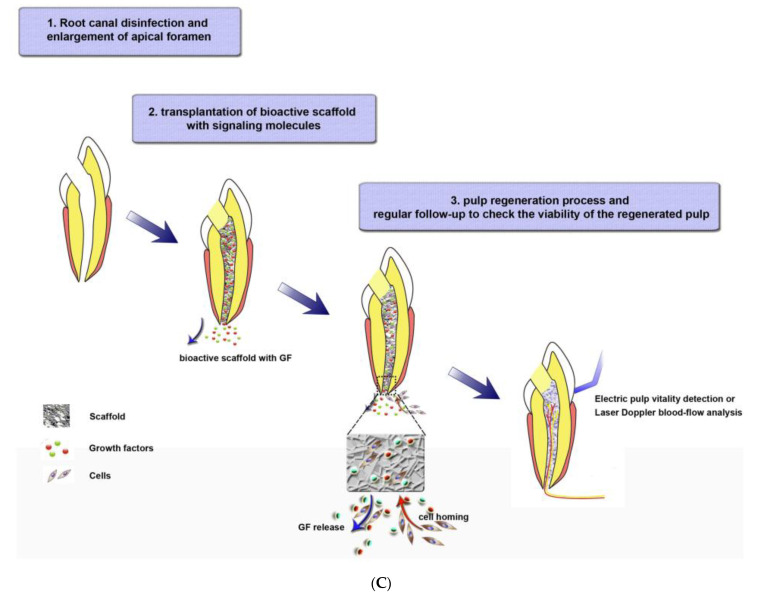
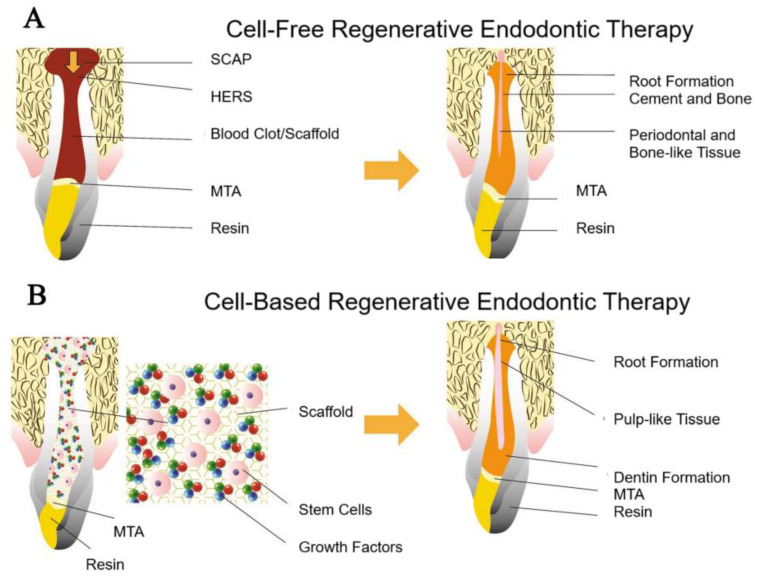
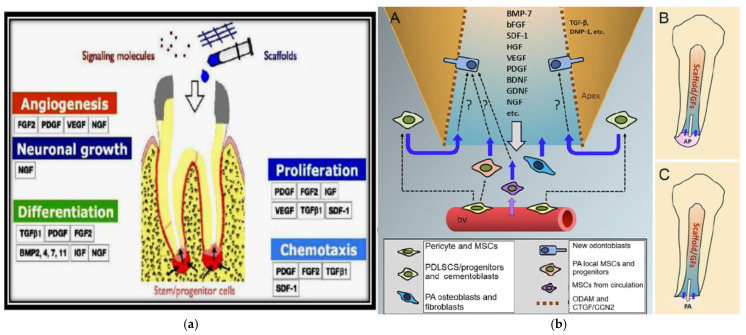
Regenerative Endodontic Therapies (RETs) offer transformative potential by leveraging polymer-based scaffolds, stem cells, and growth factors to regenerate damaged dental pulp tissue, thereby restoring tooth vitality and prolonging tooth function. While conventional treatments focus on infection control, they often compromise the structural and biological integrity of the tooth. RETs, in contrast, aim to restore the natural function of the pulp-dentin complex by promoting cellular regeneration and immune modulation. In this context, biodegradable polymers-such as collagen, gelatin methacryloyl (GelMA), and synthetic alternatives-serve as scaffolding materials that mimic the extracellular matrix, support cell attachment and proliferation, and enable localized delivery of bioactive factors. Together, the tissue engineering triad-polymer-based scaffolds, stem cells, and signaling molecules-facilitates root development, apical closure, and increased fracture resistance. Recent innovations in polymeric scaffold design, including injectable hydrogels and 3D bioprinting technologies, have enhanced clinical translation by enabling minimally invasive and patient-specific RETs. Despite progress, challenges such as immune compatibility, scaffold degradation rates, and the standardization of clinical protocols remain. RETs, thus, represent a paradigm shift in dental care, aligning with the body's intrinsic healing capacity and offering improved long-term outcomes for patients.
Keywords: 3D bioprinting; collagen; dental; dental pulp stem cells; regeneration; transforming growth factor beta.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Hydrogels and Dentin-Pulp Complex Regeneration: From the Benchtop to Clinical Translation.Polymers (Basel). 2020 Dec 9;12(12):2935. doi: 10.3390/polym12122935. Polymers (Basel). 2020. PMID: 33316886 Free PMC article. Review.
-
Bovine pulp extracellular matrix hydrogel for regenerative endodontic applications: in vitro characterization and in vivo analysis in a necrotic tooth model.Head Face Med. 2024 Oct 22;20(1):61. doi: 10.1186/s13005-024-00460-y. Head Face Med. 2024. PMID: 39438876 Free PMC article.
-
Polymer-Based Scaffolds as an Implantable Material in Regenerative Dentistry: A Review.J Funct Biomater. 2025 Feb 24;16(3):80. doi: 10.3390/jfb16030080. J Funct Biomater. 2025. PMID: 40137359 Free PMC article. Review.
-
Present and future of tissue engineering scaffolds for dentin-pulp complex regeneration.J Tissue Eng Regen Med. 2019 Jan;13(1):58-75. doi: 10.1002/term.2769. Epub 2018 Dec 17. J Tissue Eng Regen Med. 2019. PMID: 30376696 Free PMC article. Review.
-
GelMA/TCP nanocomposite scaffold for vital pulp therapy.Acta Biomater. 2024 Jan 1;173:495-508. doi: 10.1016/j.actbio.2023.11.005. Epub 2023 Nov 7. Acta Biomater. 2024. PMID: 37939819 Free PMC article.
References
-
- Boyd R.C. Wiggs’s Veterinary Dentistry: Principles and Practice. John Wiley & Sons; Hoboken, NJ, USA: 2019. Basic endodontic therapy; pp. 311–334.
-
- Al-Helou N. In: Contemporary Endodontics for Children and Adolescents. Fuks A.B., Moskovitz M., Tickotsky N., editors. Springer; Berlin, Germany: 2023.
Publication types
LinkOut - more resources
Full Text Sources
