

Lymphopenia: An early indicator of Crimean-Congo haemorrhagic fever
- PMID: 40509968
- PMCID: PMC12318437
- DOI: 10.1111/tmi.14138
Lymphopenia: An early indicator of Crimean-Congo haemorrhagic fever
Abstract
Objectives: Crimean-Congo haemorrhagic fever is a lethal tick-borne disease characterised by initially nonspecific symptoms. While thrombocytopenia and leucopenia are established diagnostic markers, there is a need for earlier indicators. This study evaluates lymphopenia as a marker for Crimean-Congo haemorrhagic fever.
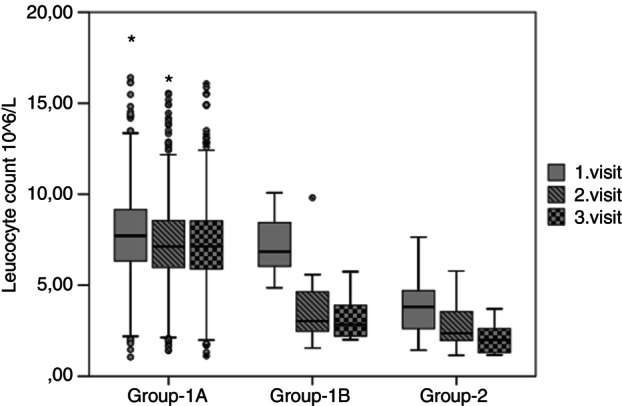
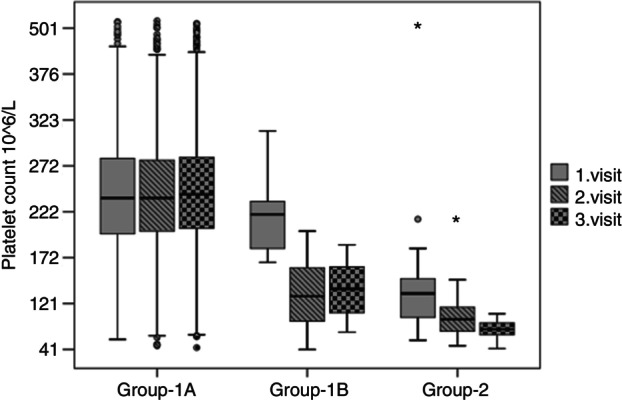
Methods: This retrospective study analysed patients admitted with arthropod bites from 2018 to 2021. Patients were classified based on initial leucocyte and platelet counts into Group 1 (normal values) and Group 2 (low values). Within Group 1, patients were classified as Group 1B if they developed thrombocytopenia and leucopenia during follow-up, whereas those with stable counts were designated as Group 1A. Variance and ROC curve analysis were used to evaluate blood counts.
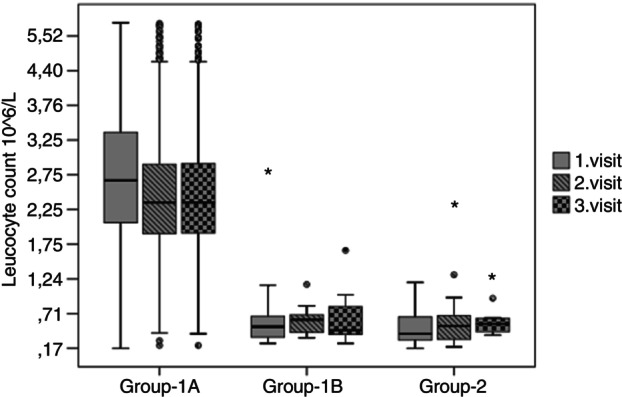
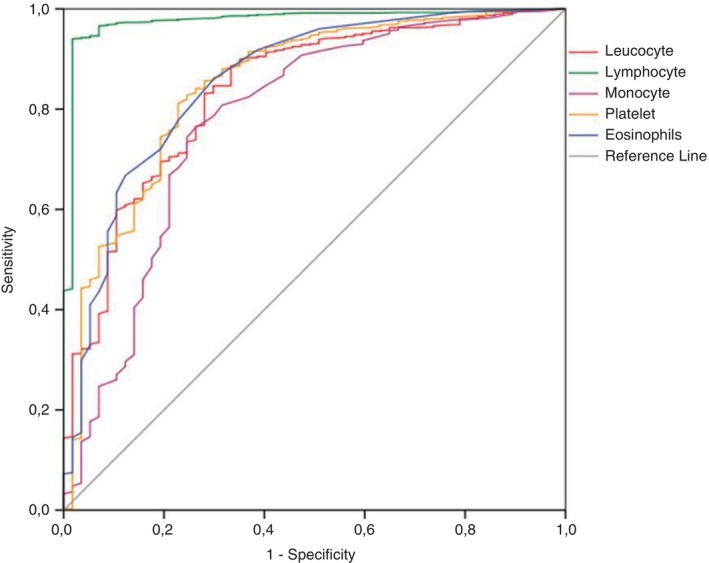
Results: Of 914 evaluated patients, 870 with normal CBCs were categorised into Group 1, and 44 with low counts into Group 2. Within Group 1, 16 patients subsequently developed thrombocytopenia and leucopenia (Group 1B), while the rest remained stable (Group 1A). All patients in Groups 1B and 2 were later confirmed to have Crimean-Congo haemorrhagic fever via RT-PCR. Initial lymphocyte counts varied significantly, with 2.7 × 109/L in Group 1A, 0.52 × 109/L in Group 1B, and 0.42 × 109/L in Group 2, with notable reductions observed in Group 1B and Group 2 (p < 0.001). ROC analysis showed lymphocyte counts below 1.19 × 109/L were the most sensitive and specific for Crimean-Congo haemorrhagic fever (area under curve is 0.976 [95% CI: 0.957-0.995]), exceeding traditional markers.
Conclusions: Lymphocyte depletion precedes changes in leucocyte and platelet counts, affirming its potential as an early diagnostic marker for Crimean-Congo haemorrhagic fever. Early detection through lymphocyte monitoring could improve patient management and reduce transmission in endemic areas.
Keywords: Crimean‐Congo haemorrhagic fever; leucopenia; lymphopenia; thrombocytopenia; tick bites.
© 2025 The Authors Tropical Medicine & International Health published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Ribavirin for treating Crimean Congo haemorrhagic fever.Cochrane Database Syst Rev. 2018 Jun 5;6(6):CD012713. doi: 10.1002/14651858.CD012713.pub2. Cochrane Database Syst Rev. 2018. PMID: 29869797 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Evaluation of the relationship between YKL-40 level and clinical severity in patients with Crimean-Congo hemorrhagic fever.Pathog Glob Health. 2024 Sep;118(6):492-498. doi: 10.1080/20477724.2024.2392225. Epub 2024 Aug 14. Pathog Glob Health. 2024. PMID: 39140475 Free PMC article.
-
Crimean-Congo haemorrhagic fever in travellers: A systematic review.Travel Med Infect Dis. 2016 Mar-Apr;14(2):73-80. doi: 10.1016/j.tmaid.2016.03.002. Epub 2016 Mar 10. Travel Med Infect Dis. 2016. PMID: 26970396 Free PMC article.
-
A case report and mini-review of Crimean-Congo hemorrhagic fever with encephalitis: an unexpected complication.J Neurovirol. 2025 Jun;31(3):197-207. doi: 10.1007/s13365-025-01253-y. Epub 2025 Apr 22. J Neurovirol. 2025. PMID: 40261581 Review.
References
-
- Günaydın NS, Aydın K, Yılmaz G, Çaylan R, Köksal İ. Crimean‐Congo hemorrhagic fever cases in the eastern Black Sea region of Turkey: demographic, geographic, climatic, and clinical characteristics. Turk J Med Sci. 2010;40(6):829–834. 10.3906/sag-0907-2 - DOI
-
- World Health Organisation . Crimean‐Congo haemorrhagic fever (CCHF) outbreak toolbox. 2022. [cited 2022 Dec 1]. Available from: https://cdn.who.int/media/docs/default-source/outbreak-toolkit/final_cch...
-
- Republic of Türkiye Ministry of Health . Crimean‐Congo hemorrhagic fever (CCHF) case management algorithm. 2015. [cited 2022 May 1]. Available from: https://hsgm.saglik.gov.tr/depo/birimler/zoonotik-ve-vektorel-hastalikla...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
