

An Imitator Within: A Case of Appendiceal Neuroma Masquerading as Chronic Appendicitis
- PMID: 40510085
- PMCID: PMC12159277
- DOI: 10.7759/cureus.83986
An Imitator Within: A Case of Appendiceal Neuroma Masquerading as Chronic Appendicitis
Abstract
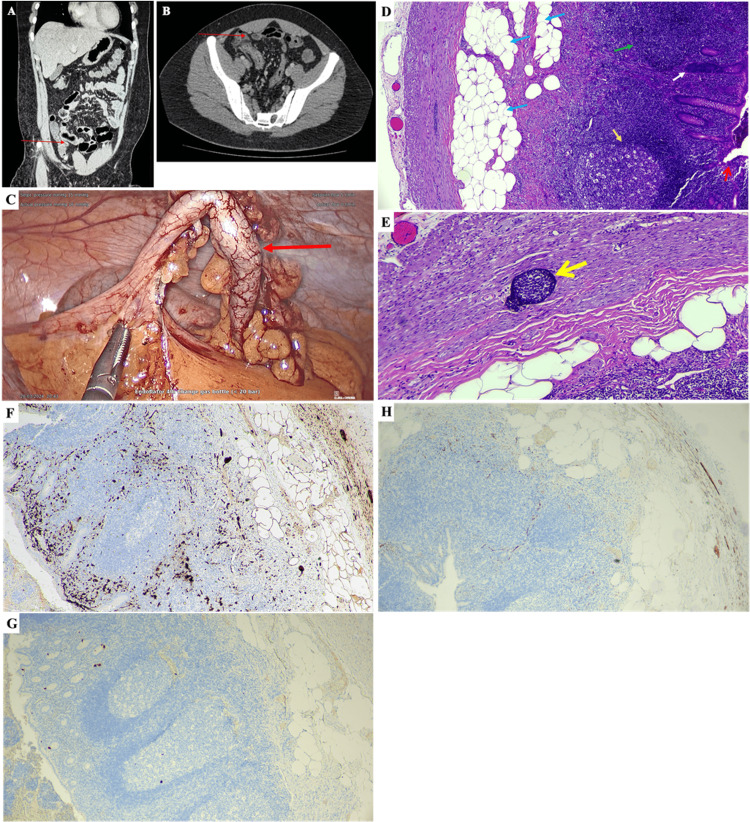
The incidence of appendicitis, an inflammation of the appendix, has been rising significantly in many countries worldwide. Appendicitis may present in various forms, including acute or chronic inflammation, and can manifest as either uncomplicated or complicated conditions, etc. Among these conditions, chronic appendicitis is a rare type of appendiceal inflammation that is less common than acute appendicitis. In this case report, we describe a case of idiopathic appendiceal neuroma, which was initially misdiagnosed as acute gastroenteritis. Diagnosis was further supported by comprehensive laboratory testing, computed tomography and ultrasound imaging, as well as immunohistochemical staining. The patient made a full recovery following a laparoscopic appendectomy. This case highlights appendiceal neuroma as an elusive entity with atypical presentation of appendicitis and chronic histological features, emphasising the critical role of histopathology in establishing a definitive diagnosis.
Keywords: appendicitis; chronic; fibrous obliteration; gastroenteritis; neuroma.
Copyright © 2025, Siew et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources