

Quantitative contrast enhancement volume on immediate post-thrombectomy CT predicts symptomatic intracranial hemorrhage and functional outcomes in acute large vessel occlusion stroke
- PMID: 40510208
- PMCID: PMC12158709
- DOI: 10.3389/fneur.2025.1579659
Quantitative contrast enhancement volume on immediate post-thrombectomy CT predicts symptomatic intracranial hemorrhage and functional outcomes in acute large vessel occlusion stroke
Abstract
Objectives: Symptomatic intracranial hemorrhage (sICH) following endovascular thrombectomy (EVT) for acute ischemic stroke due to anterior circulation large vessel occlusion (AIS-LVO) significantly impacts clinical outcomes. Contrast enhancement (CE) on immediate post-EVT non-contrast CT (NCCT) may reflect blood-brain barrier disruption, but its volumetric correlation with sICH and functional independence remains underexplored.
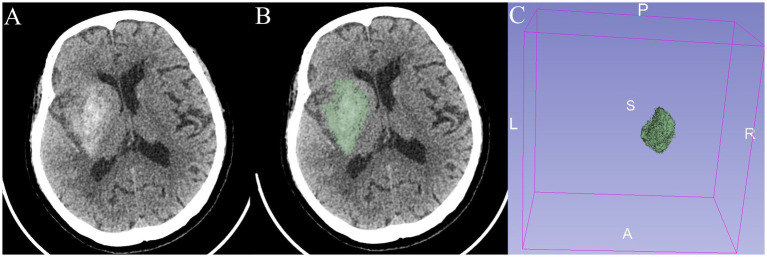
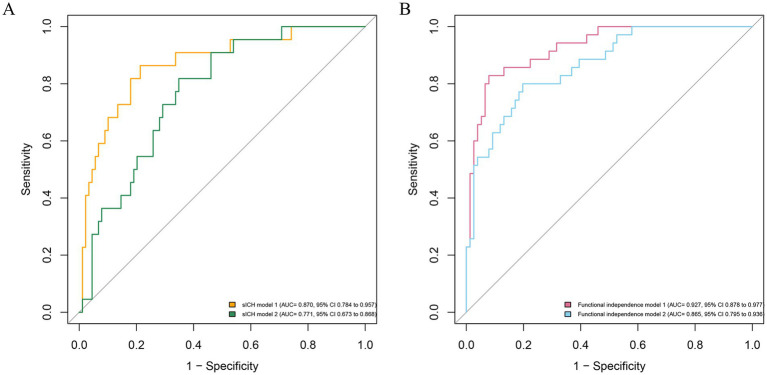
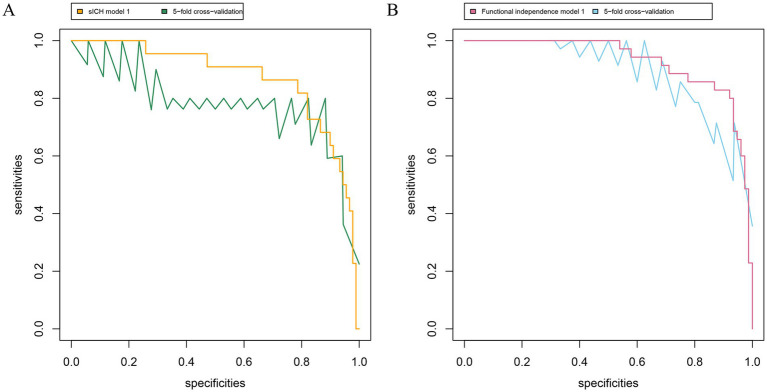
Methods: We performed a retrospective screening on consecutive AIS-LVO patients who had CE on NCCT immediately within 2 h after EVT. The quantitative volume of CE was calculated by using 3D Slicer software. Multivariable logistic regression was performed to achieve the risk factors of sICH and functional independence. The discrimination and calibration of the multivariable models were assessed using the area under the receiver operator characteristic curve, fivefold cross-validation, calibration curve, and decision curve analysis.
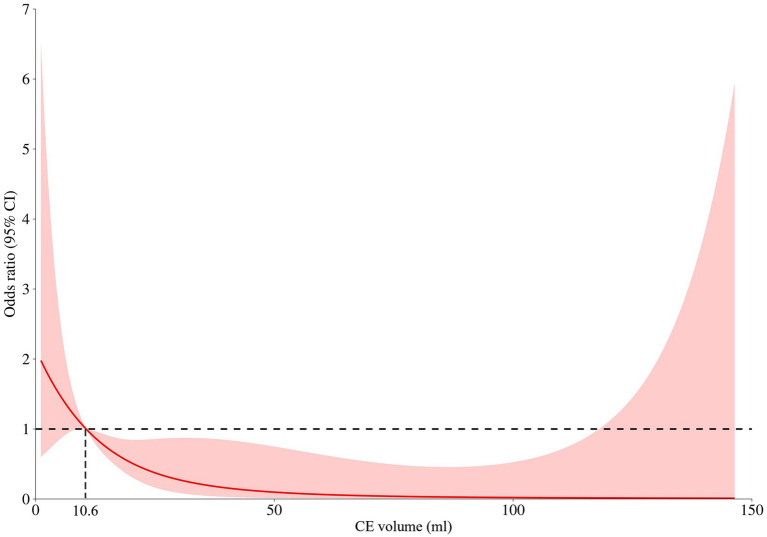
Results: In this study, 111 patients were enrolled in the final analysis. According to the restricted cubic spline, 10.6 mL was the optimal threshold of CE volume dichotomization for patients with AIS-LVO. In multivariate regression analysis, the CE+ group (CE volume beyond 10.6 mL) was significantly associated with sICH (aOR: 5.24, 95% CI: 1.45-18.99, p = 0.012) and functional independence (10.9% vs. 51.8%; aOR 0.05, 95% CI: 0.01-0.28, p < 0.001). The multivariable models demonstrated good discrimination and calibration in this cohort, as well as the fivefold cross-validation.
Conclusion: Volumetric quantification of CE on immediate post-EVT NCCT serves as a novel biomarker for early sICH risk stratification and functional prognosis in AIS-LVO. Incorporating CE volume into predictive models enhances clinical utility, enabling timely diagnosis and intervention.
Keywords: acute ischemic stroke; contrast enhancement; endovascular treatment; functional independence; symptomatic intracranial hemorrhage.
Copyright © 2025 Huang, Xiong, Gong, Jiang, Huang, Wang, Yuan, Gao, Ban, Chen and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Predicting symptomatic intracranial hemorrhage in anterior circulation stroke patients with contrast enhancement after thrombectomy: the CAGA score.J Neurointerv Surg. 2023 Dec 21;15(e3):e356-e362. doi: 10.1136/jnis-2022-019787. J Neurointerv Surg. 2023. PMID: 36627195
-
The Association of the Spatial Location of Contrast Extravasation with Symptomatic Intracranial Hemorrhage after Endovascular Therapy in Acute Ischemic Stroke Patients.Curr Neurovasc Res. 2023;20(3):354-361. doi: 10.2174/1567202620666230721101413. Curr Neurovasc Res. 2023. PMID: 37488759
-
Contrast enhancement by location and volume is associated with long-term outcome after thrombectomy in acute ischemic stroke.Sci Rep. 2022 Oct 10;12(1):16998. doi: 10.1038/s41598-022-21276-3. Sci Rep. 2022. PMID: 36216846 Free PMC article.
-
Brain imaging prior to thrombectomy in the late window of large vessel occlusion ischemic stroke: a systematic review and meta-analysis.Neuroradiology. 2024 May;66(5):809-816. doi: 10.1007/s00234-024-03324-z. Epub 2024 Mar 1. Neuroradiology. 2024. PMID: 38427071
-
Endovascular thrombectomy vs best medical management for late presentation acute ischaemic stroke with large vessel occlusion without CT perfusion or MR imaging selection: A systematic review and meta-analysis.J Stroke Cerebrovasc Dis. 2024 Nov;33(11):108002. doi: 10.1016/j.jstrokecerebrovasdis.2024.108002. Epub 2024 Sep 7. J Stroke Cerebrovasc Dis. 2024. PMID: 39245396
References
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early Management of Patients with Acute Ischemic Stroke: 2019 update to the 2018 guidelines for the early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211, PMID: - DOI - PubMed
-
- Zi W, Qiu Z, Li F, Sang H, Wu D, Luo W, et al. Effect of endovascular treatment alone vs intravenous Alteplase plus endovascular treatment on functional Independence in patients with acute ischemic stroke: the DEVT randomized clinical trial. JAMA. (2021) 325:234–43. doi: 10.1001/jama.2020.23523, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources