

The interactions of Lipoprotein(a) with common cardiovascular risk factors in cardiovascular disease risk: evidence based on the UK Biobank
- PMID: 40510257
- PMCID: PMC12162037
- DOI: 10.1016/j.ajpc.2025.101008
The interactions of Lipoprotein(a) with common cardiovascular risk factors in cardiovascular disease risk: evidence based on the UK Biobank
Abstract
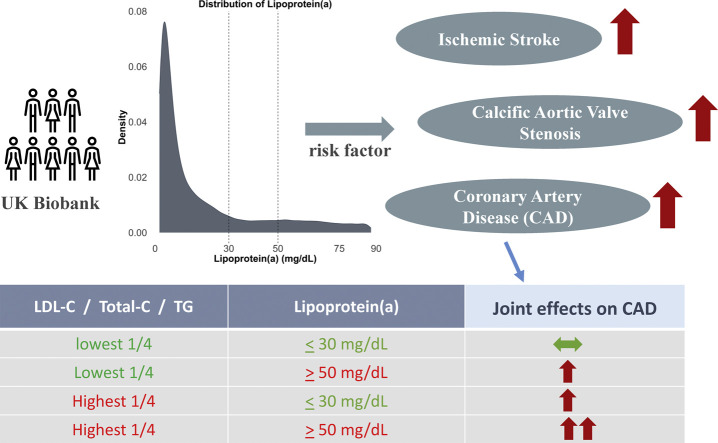
Background: : Although Lipoprotein(a) (Lp(a)) is associated with cardiovascular disease, it is unclear whether the associated risk is similar in the presence of other concomitant risk factors. Here, we aimed to investigate the interactions between Lp(a) and common cardiovascular risk factors on coronary artery disease (CAD), calcific aortic valve stenosis (CAVS) and ischemic stroke (IS).
Methods: : We included 127,958 unrelated European-ancestry participants from UK Biobank (54.7 % women) with data available on Lp(a) and without a baseline history of CAD, CAVS and IS. Multivariable-adjusted Cox proportional hazards interaction models were used to study whether the associations of Lp(a) with outcomes varied based on the level of total cholesterol (Total-C), low-density lipoprotein-cholesterol (LDL-C), triglycerides (TG) and other cardiovascular risk factors.
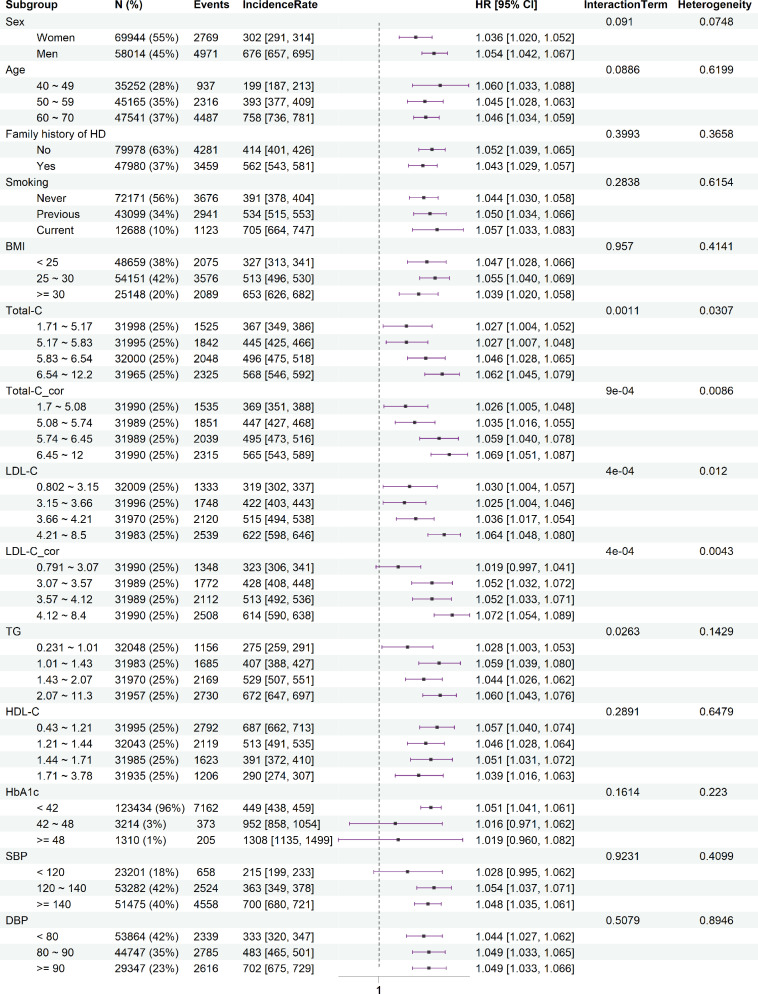
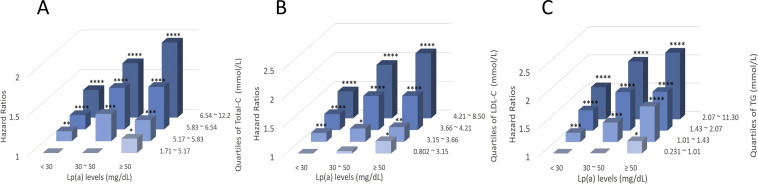
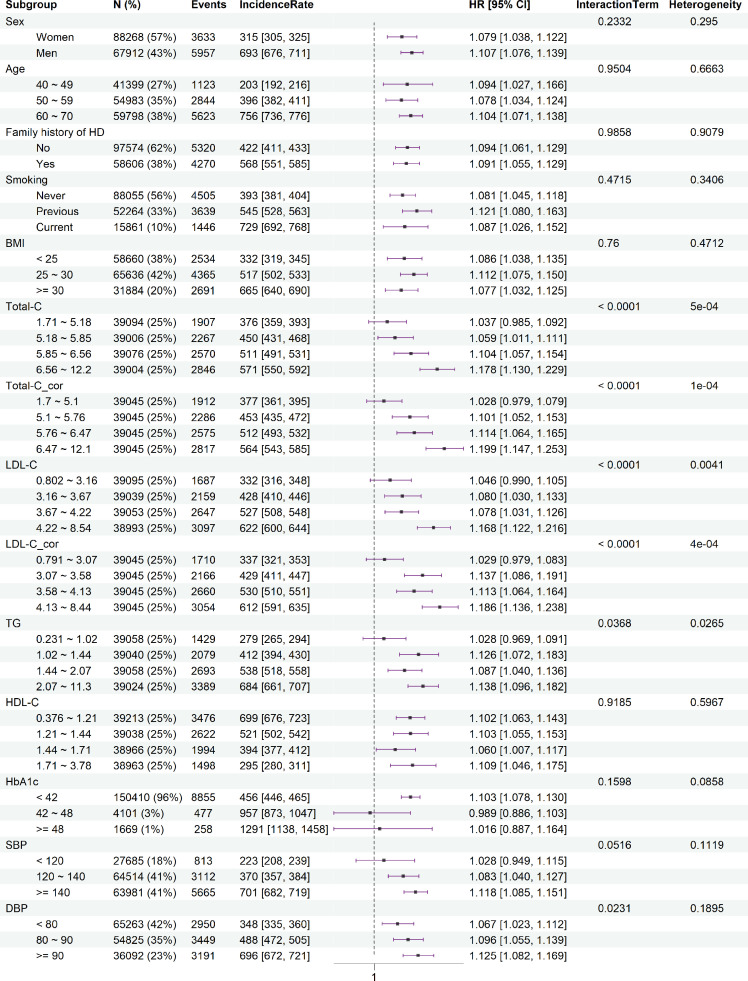
Results: : Higher Lp(a) levels were associated with higher risks of CAD, CAVS and IS. Per 10 mg/dL increase in Lp(a), hazard ratios [95 % confidence interval] were 1.05 [1.04, 1.06], 1.06 [1.04, 1.09], and 1.01 [0.99, 1.03] for CAD, CAVS and IS, respectively. For CAD, interactions were observed between Lp(a) and Total-C (Pinteraction =0.001), LDL-C (Pinteraction =4e-4) and TG (Pinteraction =0.026). In more detail, participants with Lp(a) ≥ 50 mg/dL in the highest quartile of Total-C, LDL-C and TG showed evidence of additive interaction in CAD, with relative excess risk due to interaction (RERI) of 0.42 (0.17, 0.67), 0.44 (0.18, 0.71), and 0.39 (0.12, 0.67), respectively. No such interactions were observed in CAVS and IS.
Conclusions: Lp(a)-associated CAD risk seems to particularly affect those having levels of Total-C, LDL-C and TG above the thresholds from clinical guidelines.
Keywords: Calcific aortic valve stenosis; Common cardiovascular risk factors; Coronary artery disease; Interaction effects; Lipoprotein(a) risk.
© 2025 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Genetic Variation in LPA, Calcific Aortic Valve Stenosis in Patients Undergoing Cardiac Surgery, and Familial Risk of Aortic Valve Microcalcification.JAMA Cardiol. 2019 Jul 1;4(7):620-627. doi: 10.1001/jamacardio.2019.1581. JAMA Cardiol. 2019. PMID: 31141105 Free PMC article.
-
Sex-Specific Associations of Genetically Predicted Circulating Lp(a) (Lipoprotein(a)) and Hepatic LPA Gene Expression Levels With Cardiovascular Outcomes: Mendelian Randomization and Observational Analyses.Circ Genom Precis Med. 2021 Aug;14(4):e003271. doi: 10.1161/CIRCGEN.120.003271. Epub 2021 Jul 19. Circ Genom Precis Med. 2021. PMID: 34279996
-
Interaction of Autotaxin With Lipoprotein(a) in Patients With Calcific Aortic Valve Stenosis.JACC Basic Transl Sci. 2020 Aug 26;5(9):888-897. doi: 10.1016/j.jacbts.2020.06.012. eCollection 2020 Sep. JACC Basic Transl Sci. 2020. PMID: 33015412 Free PMC article.
-
Lipoprotein(a) as a Causal Risk Factor for Cardiovascular Disease.Curr Cardiovasc Risk Rep. 2025;19(1):8. doi: 10.1007/s12170-025-00760-1. Epub 2025 Feb 18. Curr Cardiovasc Risk Rep. 2025. PMID: 39980866 Free PMC article. Review.
-
Lipoprotein(a) and Cardiovascular Disease in Chinese Population: A Beijing Heart Society Expert Scientific Statement.JACC Asia. 2022 Nov 15;2(6):653-665. doi: 10.1016/j.jacasi.2022.08.015. eCollection 2022 Nov. JACC Asia. 2022. PMID: 36444328 Free PMC article. Review.
References
-
- Kåre Berg. A NEW SERUM TYPE SYSTEM IN MAN—THE lp SYSTEM. Acta Pathol Microbiol Scand. 1963;59(3):369–382. - PubMed
-
- Duarte Lau F., Giugliano R.P. Lipoprotein(a) and its significance in cardiovascular disease: A review. JAMA Cardiol. 2022;7(7):760–769. - PubMed
-
- Grundy S.M., Stone N.J., Bailey A.L., Beam C., Birtcher K.K., Blumenthal R.S., et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood Cholesterol: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice guidelines. J Am Coll Cardiol. 2019;73(24):3168–3209. - PubMed
-
- Pearson G.J., Thanassoulis G., Anderson T.J., Barry A.R., Couture P., Dayan N., et al. 2021 Canadian Cardiovascular Society Guidelines for the management of dyslipidemia for the prevention of Cardiovascular disease in adults. Can J Cardiol. 2021;37(8):1129–1150. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
