

Cardiovascular and Thromboembolic Events in Children and Adults With Glomerular Disease: Findings From the Cure GlomeruloNephropathy (CureGN) Network
- PMID: 40510608
- PMCID: PMC12152344
- DOI: 10.1016/j.xkme.2024.100877
Cardiovascular and Thromboembolic Events in Children and Adults With Glomerular Disease: Findings From the Cure GlomeruloNephropathy (CureGN) Network
Abstract
Rationale & objective: Cardiovascular (CV) and thromboembolic (TE) events are known complications of glomerular disease (GD), but their incidence and risk factors are poorly characterized. This analysis describes CV and TE outcomes in the Cure GlomeruloNephropathy (CureGN) Network.
Study design: Prospective cohort study.
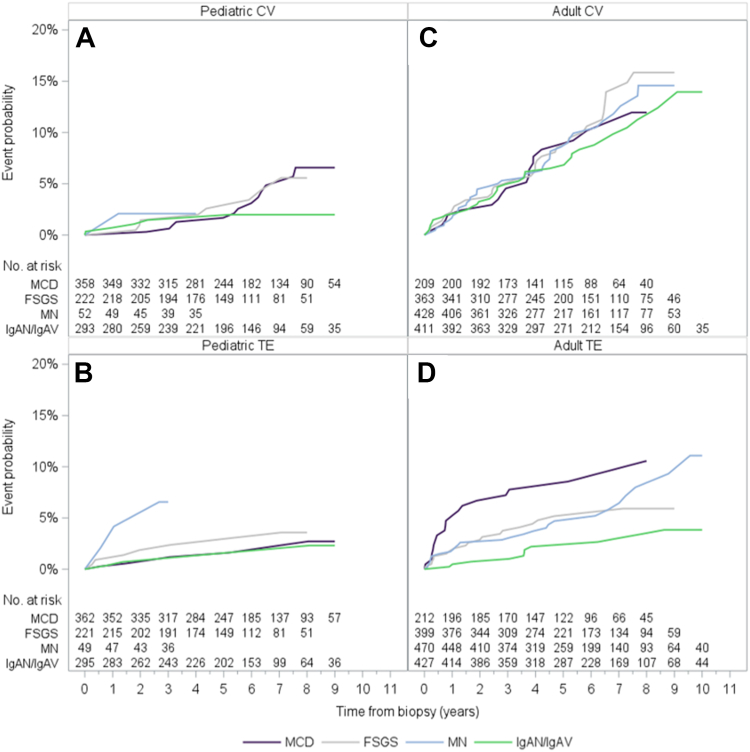
Setting & participants: CureGN is a prospective cohort study of children and adults with biopsy-proven minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS), membranous nephropathy (MN), or IgA nephropathy (IgAN)/vasculitis (IgAV). Data from 2,545 children and adults (23% MCD, 23% MN, 25% FSGS, 29% IgAN/IgAV) was analyzed.
Exposure: Estimated glomerular filtration rate (eGFR), proteinuria, serum albumin, tobacco use, body mass index, hypertension, renin-angiotensin-aldosterone system.
Outcomes: CV and TE events.
Analytic approach: Kaplan-Meier curves were used to estimate cumulative incidence, and multivariable Cox proportional hazards models were fitted to estimate associations of histologic diagnosis, age, biological sex, and race. Laboratory and other clinical data were evaluated separately in models adjusted for base model covariates.
Results: Median follow-up time was 4.6 years (IQR 2.7-6.1). The cumulative incidence of first CV and TE event postbiopsy was 3% and 2% in children and 10% and 5% in adults, respectively. No association between GD subtype and risk of CV or TE event was detected. Older age and Black race were associated with higher risk of first CV and TE event {hazard ratio (HR) (95% confidence interval {CI}) per 5 years, CV = 1.17 (1.12-1.23); TE = 1.11 (1.05-1.18); for Black race, CV = 1.62 (1.03-2.56), TE = 2.25 (1.27-4.01)}. Lower eGFR, higher urinary protein-creatinine ratio (UPCR), and lower serum albumin levels at enrollment were associated with higher risk of first CV and TE event (eGFR per 10 mL/min/1.73 m2, CV = 0.87 [0.81-0.93], TE = 0.80 [0.73-0.88]; UPCR per mg/mg, CV = 1.04 [1.02-1.07], TE = 1.03 [1.00-1.07]; serum albumin per g/dL, CV = 0.75 [0.59-0.95], TE = 0.71 [0.53-0.96]).
Limitations: Age of cohort, duration of follow-up.
Conclusions: In the CureGN cohort, elevated risk of incident CV and TE events is associated with severity of kidney disease rather than GD subtype.
Keywords: Cardiovascular; glomerular disease; thromboembolic.
Plain language summary
Individuals with glomerular disease are at risk for cardiovascular and thromboembolic events. The aim of our study was to determine the frequency and risk factors for such events in adults and children with minimal change disease, focal segmental glomerulosclerosis, membranous nephropathy, and IgA nephropathy/vasculitis enrolled in the CureGN study. Our ultimate goal is to equip physicians with tools to identify high-risk individuals and help develop mitigative therapies. We found that poor kidney function, low serum albumin level, and high levels of urine protein at the time participants entered the study, along with older age and self-reported Black race were associated with a higher risk of both cardiovascular and thromboembolic events. In addition, these risk factors are more important than the specific type of glomerular disease.
© 2024 The Authors.
Figures



References
-
- Canney M., Gunning H.M., Zheng Y., et al. The risk of cardiovascular events in individuals with primary glomerular diseases. Am J Kidney Dis. 2022;80(6):740–750. - PubMed
-
- Go A.S., Chertow G.M., Fan D., McCulloch C.E., Hsu C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. - PubMed
-
- Klausen K., Borch-Johnsen K., Feldt-Rasmussen B., et al. Very low levels of microalbuminuria are associated with increased risk of coronary heart disease and death independently of renal function, hypertension, and diabetes. Circulation. 2004;110(1):32–35. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
