

The sternum in detail: a review of the anatomy and pathologies of the sternum
- PMID: 40510691
- PMCID: PMC12160079
- DOI: 10.1590/0100-3984.2024.0128-en
The sternum in detail: a review of the anatomy and pathologies of the sternum
Abstract
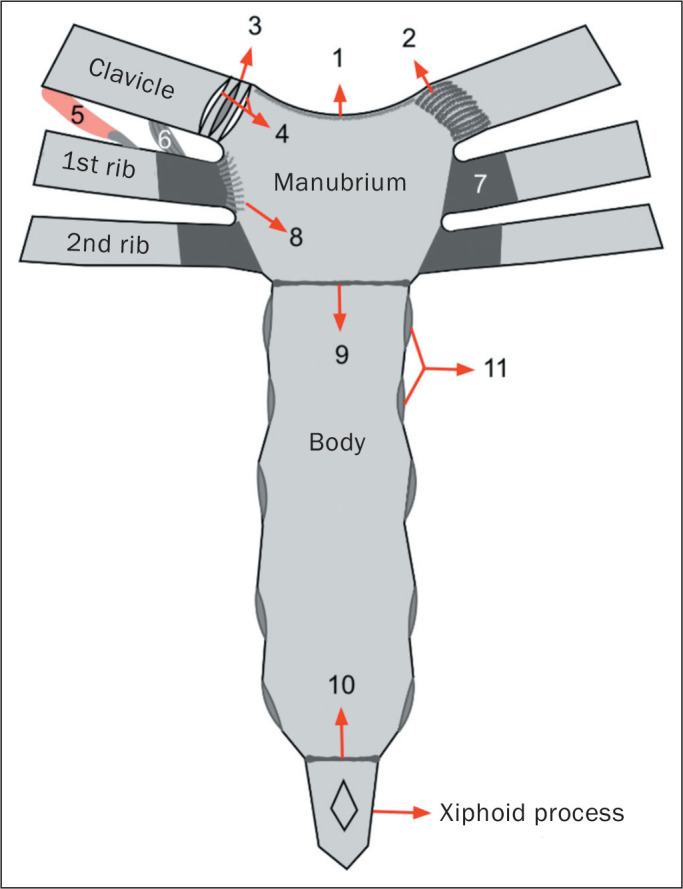
The sternum and the sternoclavicular joints can exhibit a wide range of anatomical variations and serve as sites for numerous diseases, many of which are diagnosed solely through imaging studies. Recognizing these variations and differentiating them from pathological conditions is essential for radiologists, because accurate identification helps prevent misdiagnoses and treatment delays. This study provides a comprehensive review of the sternal anatomy, addressing anatomical variations, as well as mechanical, inflammatory, and traumatic pathologies, discussing their radiographic characteristics across different imaging modalities. Thus, it provides an overview of the key radiological findings.
O esterno e as articulações esternoclaviculares podem apresentar ampla gama de variações anatômicas e ser sítios de diferentes doenças, muitas das quais diagnosticadas somente por meio de exames de imagem. Reconhecer essas variações e diferenciá-las de condições patológicas é essencial para o radiologista, uma vez que a identificação precisa pode evitar diagnósticos errôneos e atrasos no tratamento. Este estudo revisa a anatomia do esterno, abordando as variações anatômicas, as patologias mecânicas, inflamatórias e traumáticas, e discute suas características radiográficas nas diferentes modalidades de imagem, proporcionando uma revisão dos seus principais achados radiológicos relevantes.
Keywords: Magnetic resonance imaging; Manubrium; Multidetector computed tomography; Sternum; X-Rays; Xiphoid bone.
Figures

Similar articles
-
Evaluation of the postnatal development of the sternum and sternal variations using multidetector CT.Diagn Interv Radiol. 2014 Jan-Feb;20(1):82-9. doi: 10.5152/dir.2013.13121. Diagn Interv Radiol. 2014. PMID: 24100061 Free PMC article.
-
Frequency of sternal variations and anomalies in living individuals evaluated by MDCT.Eur J Radiol. 2021 Sep;142:109828. doi: 10.1016/j.ejrad.2021.109828. Epub 2021 Jun 24. Eur J Radiol. 2021. PMID: 34280594 Review.
-
Anatomical variations of the sternum: sternal foramen and variant xiphoid morphology in dried adult human sternum in Ethiopia.F1000Res. 2023 Aug 7;12:934. doi: 10.12688/f1000research.133151.1. eCollection 2023. F1000Res. 2023. PMID: 38845617 Free PMC article.
-
Evaluation of the morphological characteristic and sex differences of sternum by multi-detector computed tomography.Folia Morphol (Warsz). 2018;77(3):489-497. doi: 10.5603/FM.a2018.0002. Epub 2018 Jan 18. Folia Morphol (Warsz). 2018. PMID: 29345718 Clinical Trial.
-
Imaging appearances of the sternum and sternoclavicular joints.Radiographics. 2009 May-Jun;29(3):839-59. doi: 10.1148/rg.293055136. Radiographics. 2009. PMID: 19448119 Review.
References
-
- Drake RL, Vogl AW, Mitchel AWM. Gray’s Anatomia para estudantes. 3ª. Rio de Janeiro: Elsevier Editora Ltda; 2015.
-
- Restrepo CS, Martinez S, Lemos DF, et al. Imaging appearances of the sternum and sternoclavicular joints. Radiographics. 2009;29:839–859. - PubMed
-
- Goodman LR, Teplick SK, Kay H. Computed tomography of the normal sternum. AJR Am J Roentgenol. 1983;141:219–223. - PubMed
-
- Stark P, Jaramillo D. CT of the sternum. AJR Am J Roentgenol. 1986;147:72–77. - PubMed
-
- Brossmann J, Stabler A, Preidler KW, et al. Sternoclavicular joint: MR imaging-anatomic correlation. Radiology. 1996;198:193–198. - PubMed
LinkOut - more resources
Full Text Sources