

Practice variations in indication, timing and outcome of Multiple Myeloma patients undergoing surgery for vertebral lesions - results from the European M2Spine study group
- PMID: 40512280
- PMCID: PMC12263761
- DOI: 10.1007/s11060-025-05085-y
Practice variations in indication, timing and outcome of Multiple Myeloma patients undergoing surgery for vertebral lesions - results from the European M2Spine study group
Abstract
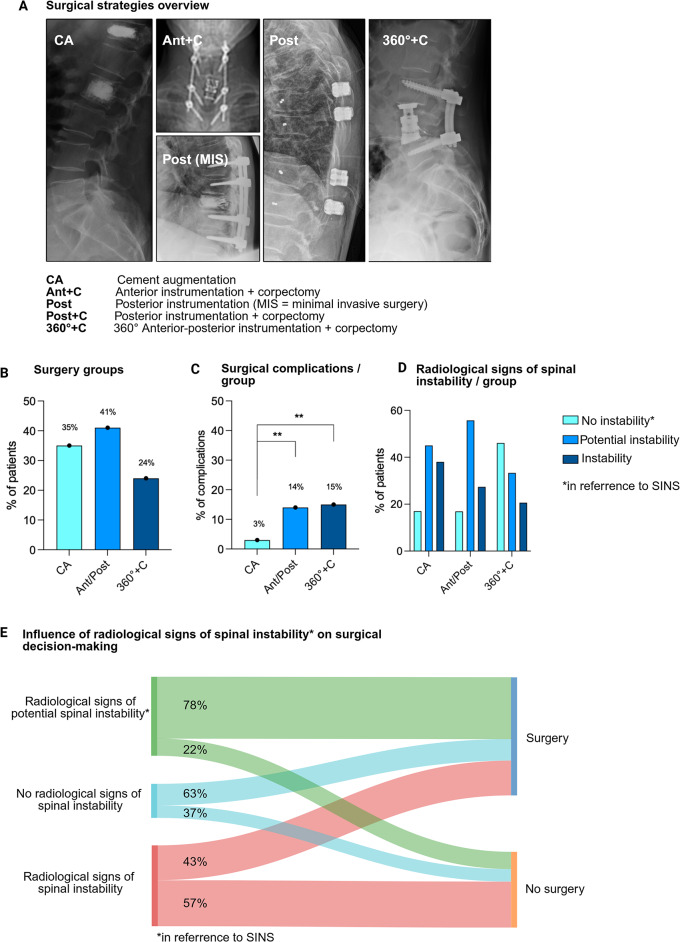
Purpose: Painful vertebral lesions are pathognomonic in Multiple Myeloma (MM). While non-surgical management is generally preferred, some patients ultimately require surgical intervention. Here we describe the largest European cohort of MM patients with vertebral lesions to examine the practice variations of spine surgery in means of indication, timing and outcome.
Methods: This study included patients with MM vertebral lesions enrolled in the European M2Spine Registry (DRKS00033326) at seven European academic spine centers between 2005 and 2023. Retrospective analysis evaluated epidemiological, clinical, and oncological treatment, focused on surgical management. Uni- and multivariate analyses identified factors associated with a decision towards spine surgery, including transitions from initially intended non-surgical approaches.
Results: 704 patients were enrolled and 493 (70%) surgically treated. Main indications for surgery were refractory vertebral pain (41%) and neurological deficits (22%). Radiological and clinical parameters indicating spinal instability as assessed retrospectively were present in 32% but associated with surgical management in only 43%. 338 patients (48%) underwent surgery during early disease stage, while 110 (16%) received delayed surgery (median: 42 months, range: 12-306 months). Statistical analysis revealed lower MM grading (ISS) at diagnosis (p < 0.001), and a new onset of neurological deficits (p < 0.001) as the most significant indicators for a cross-over from intended non-surgical to surgical treatment. Of the 78% of patients available for neurological follow up, 94% of surgically treated patients showed an improved or stable neurological status after a median of 45 months.
Conclusion: Surgical intervention proved to be a viable option for patients with refractory pain and neurological deficits. Data from future prospective studies are necessary to evaluate the clinical trajectory of surgical and non-surgical treatment, and to ultimately provide evidence-based surgical treatment guidelines for MM patients.
Keywords: Chronic vertebral pain; Multiple myeloma; Surgical complications; Surgical decision-making; Vertebral column lesions.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Ethical approval was obtained (EA4/063/20). Previous presentations: Parts of this work were presented at the Annual Congress of the German Spine Society (DWG) 2024, Nov 27-29, in Hamburg, Germany. Competing interests: The authors declare no competing interests.
Figures


References
-
- Callander NS, Baljevic M, Adekola K et al (2022) NCCN Guidelines® insights: multiple myeloma, version 3.2022. J Natl Compr Canc Netw 20(1):8–19. 10.6004/JNCCN.2022.0002 - PubMed
-
- Amelot A, Moles A, Cristini J et al (2016) Predictors of survival in patients with surgical spine multiple myeloma metastases. Surg Oncol 25(3):178–183. 10.1016/j.suronc.2016.05.012 - PubMed
-
- Gokaraju K, Butler JS, Benton A, Suarez-Huerta ML, Selvadurai S, Molloy S (2016) Multiple myeloma presenting with acute bony spinal cord compression and mechanical instability successfully managed nonoperatively. Spine J 16(8):e567–e570. 10.1016/j.spinee.2016.03.011 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
