

Computed Tomography Perfusion and Angiography for Death by Neurologic Criteria
- PMID: 40512483
- PMCID: PMC12166499
- DOI: 10.1001/jamaneurol.2025.2375
Computed Tomography Perfusion and Angiography for Death by Neurologic Criteria
Abstract
Importance: Accurate and timely confirmation of death by neurologic criteria (DNC) is essential for clinical decision-making and organ-donation processes, yet currently available ancillary tests have suboptimal diagnostic performance or limited validation.
Objectives: To determine the diagnostic accuracy, interrater reliability, and safety of brain computed tomography (CT) perfusion and CT angiography as ancillary investigations for DNC.
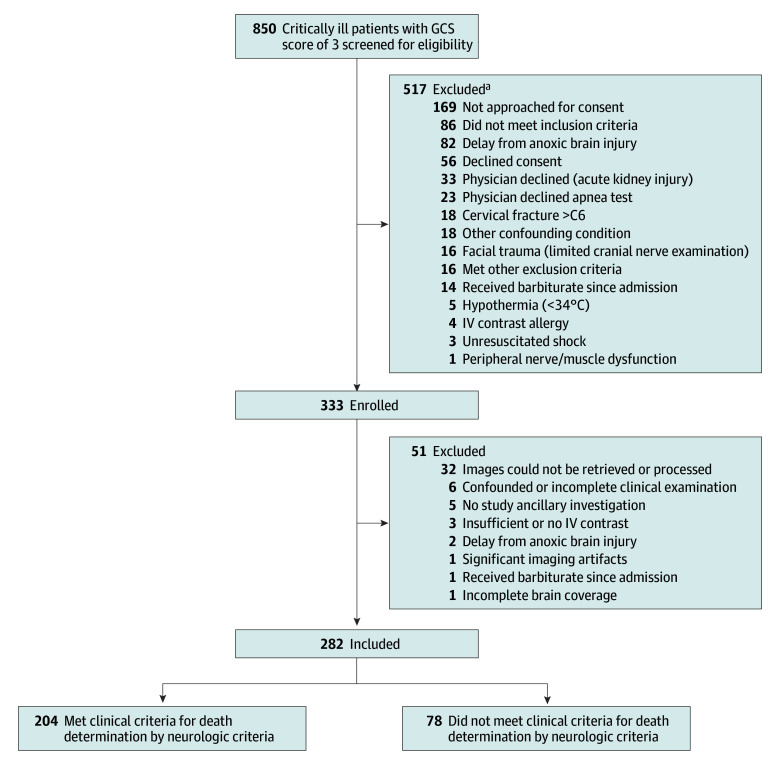
Design, setting, and participants: Between April 25, 2017, and March 10, 2021, a prospective, multicenter, blinded diagnostic accuracy cohort study was conducted in 15 adult intensive care units across Canada. Consecutive, critically ill adults (aged ≥18 years) with a Glasgow Coma Scale score of 3 and no confounding factors who were at high risk of DNC were included. Data collection and analysis were performed from April 2021 to July 2024.
Exposure: Contrast-enhanced brain CT perfusion with CT angiography reconstructions performed within 2 hours of a blinded, standardized clinical DNC examination.
Main outcomes and measures: The primary outcomes were the sensitivity and specificity of qualitative and quantitative brainstem CT perfusion for DNC determination, assessed by 2 independent neuroradiologists blinded to clinical findings; the prespecified validation threshold was greater than 98%. Secondary outcomes were the diagnostic accuracy of whole-brain CT perfusion and CT angiography, interrater reliability (Cohen κ), and adverse events associated with imaging.
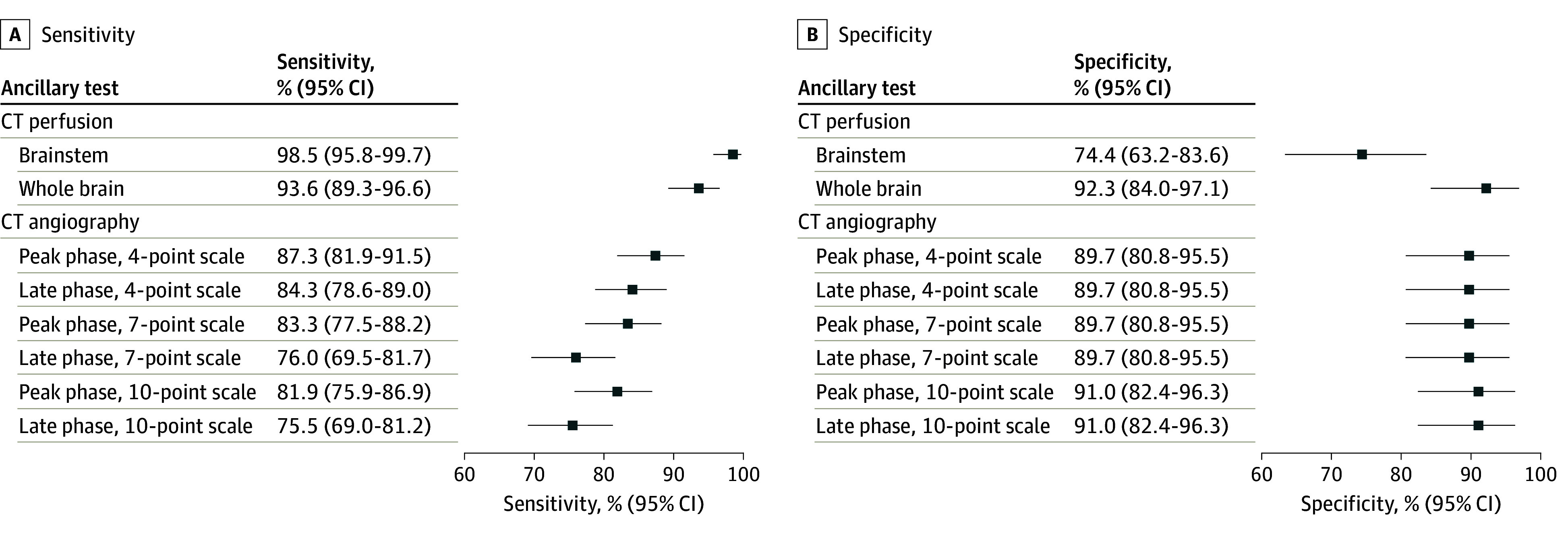
Results: A total of 282 patients (mean [SD] age, 57.8 [15.4] years; 133 [47%] female) completed the study protocol and were included in the primary analysis; 204 (72%) of these were ultimately declared deceased by standardized clinical criteria. Qualitative brainstem CT perfusion showed a sensitivity of 98.5% (95% CI, 95.8%-99.7%) and a specificity of 74.4% (95% CI, 63.2%-83.6%); quantitative brainstem CT perfusion was not diagnostically accurate. Qualitative whole-brain CT perfusion yielded a sensitivity of 93.6% (95% CI, 89.3%-96.6%) and a specificity of 92.3% (95% CI, 84.0%-97.1%). CT angiography sensitivity ranged from 75.5% (95% CI, 69.0%-81.2%) to 87.3% (95% CI, 81.9%-91.5%), and its specificity ranged from 89.7% (95% CI, 80.8%-95.5%) to 91.0% (95% CI, 82.4%-96.3%). Interrater reliability was excellent for all ancillary tests (κ ranged from 0.81 [95% CI, 0.73-0.89] to 0.84 [95% CI, 0.78-0.91]). Fourteen patients (5%) experienced minor, self-limited adverse events; no serious adverse events occurred.
Conclusions and relevance: The observed sensitivity and specificity measures for CT perfusion and CT angiography as an ancillary test for DNC did not meet the prespecified validation threshold of greater than 98%. Clinical examination remains the cornerstone of DNC, and ancillary imaging should be interpreted cautiously within a comprehensive clinical assessment.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
