

Predictive value of preclinical models for CAR-T cell therapy clinical trials: a systematic review and meta-analysis
- PMID: 40514065
- PMCID: PMC12164627
- DOI: 10.1136/jitc-2025-011698
Predictive value of preclinical models for CAR-T cell therapy clinical trials: a systematic review and meta-analysis
Abstract
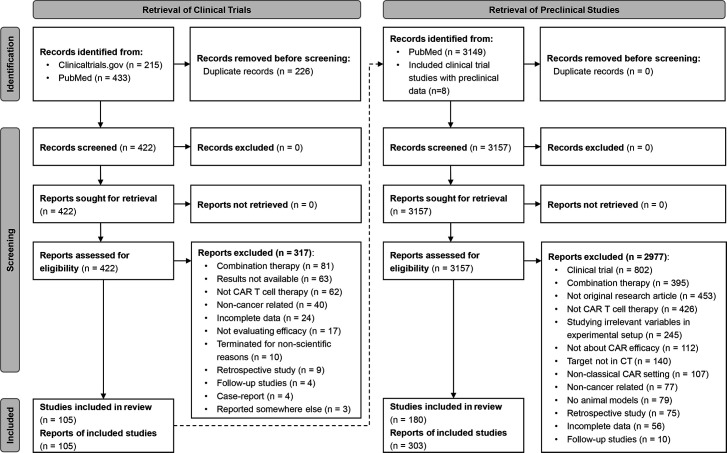
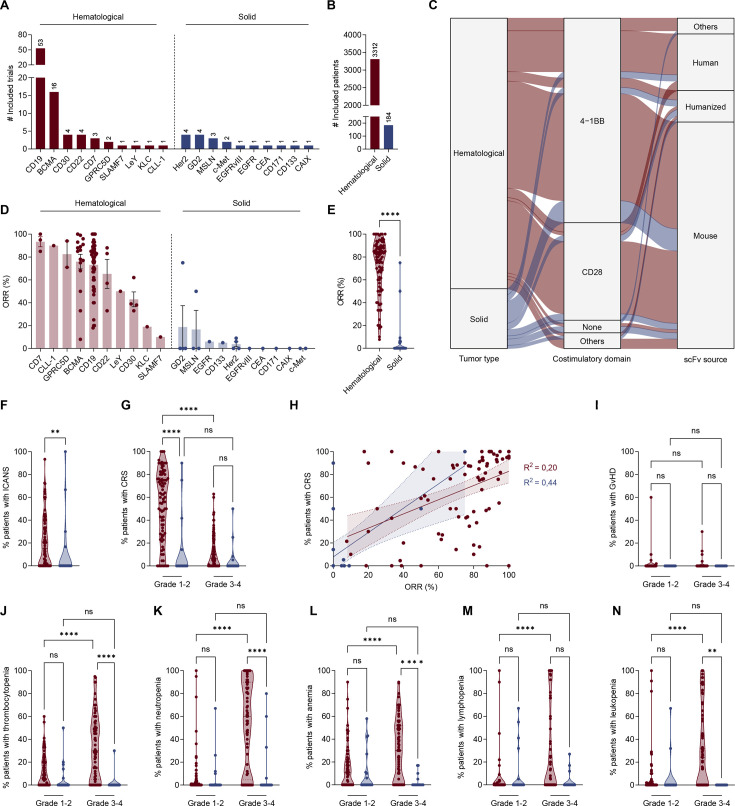
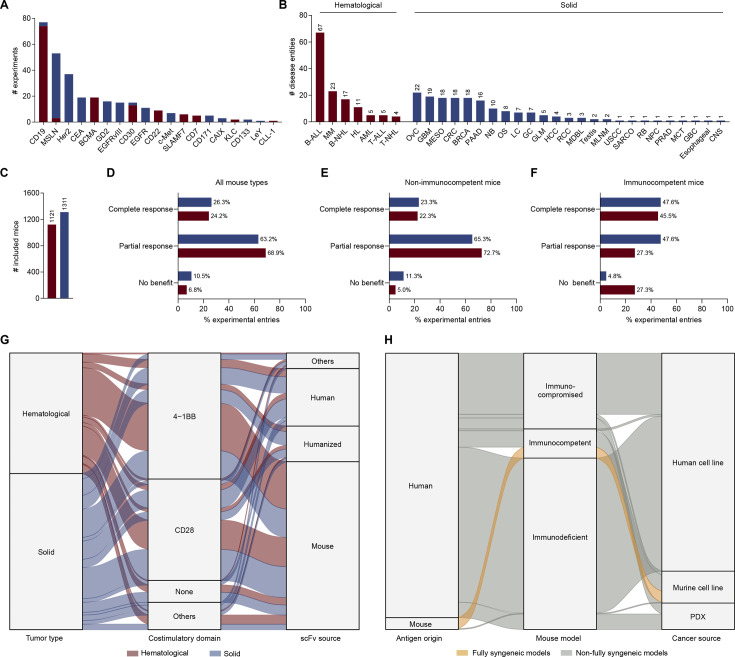
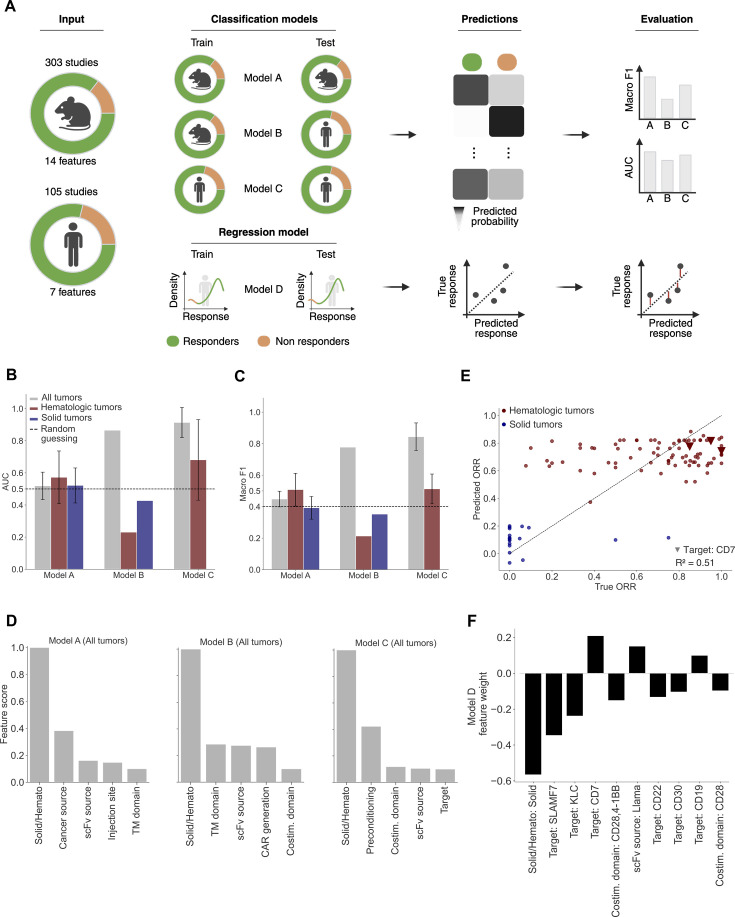
Background Experimental mouse models are indispensable for the preclinical development of cancer immunotherapies, whereby complex interactions in the tumor microenvironment can be somewhat replicated. Despite the availability of diverse models, their predictive capacity for clinical outcomes remains largely unknown, posing a hurdle in the translation from preclinical to clinical success. Methods This study systematically reviews and meta-analyzes clinical trials of chimeric antigen receptor (CAR)-T cell monotherapies with their corresponding preclinical studies. Adhering to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a comprehensive search of PubMed and ClinicalTrials.gov was conducted, identifying 422 clinical trials and 3,157 preclinical studies. From these, 105 clinical trials and 180 preclinical studies, accounting for 44 and 131 distinct CAR constructs, respectively, were included. Results Patients' responses varied based on the target antigen, expectedly with higher efficacy and toxicity rates in hematological cancers. Preclinical data analysis revealed homogeneous and antigen-independent efficacy rates. Our analysis revealed that only 4% (n=12) of mouse studies used syngeneic models, highlighting their scarcity in research. Three logistic regression models were trained on CAR structures, tumor entities, and experimental settings to predict treatment outcomes. While the logistic regression model accurately predicted clinical outcomes based on clinical or preclinical features (Macro F1 and area under the curve (AUC)>0.8), it failed in predicting preclinical outcomes from preclinical features (Macro F1<0.5, AUC<0.6), indicating that preclinical studies may be influenced by experimental factors not accounted for in the model. Conclusion These findings underscore the need to better understand the experimental factors enhancing the predictive accuracy of mouse models in preclinical settings.
Keywords: Chimeric antigen receptor - CAR; Hematologic Malignancies; META-ANALYSIS; Solid tumor; T cell.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: DA-S, LG, EC and DS declare no competing interests and have performed this work as part of their doctoral thesis. SK has received honoraria from Plectonic GmBH, TCR2 Inc., Miltenyi, Galapagos, Cymab, Novartis, BMS and GSK. SK is an inventor of several patents in the field of immuno-oncology. SK received license fees from TCR2 Inc and Carina Biotech. SK received research support from TCR2 Inc., Tabby Therapeutics, Catalym GmbH, Plectonic GmbH and Arcus Bioscience for work unrelated to the manuscript. All other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical