

Out-of-pocket expenditure and financial risks associated with treatment of chronic kidney disease in Ethiopia: a prospective cohort costing analysis
- PMID: 40514216
- PMCID: PMC12164608
- DOI: 10.1136/bmjgh-2025-019074
Out-of-pocket expenditure and financial risks associated with treatment of chronic kidney disease in Ethiopia: a prospective cohort costing analysis
Abstract
Introduction: In Ethiopia, most healthcare expenditures are paid out-of-pocket (OOP), while the burden of kidney disease (KD) is rapidly increasing, posing a major public health challenge in low- and middle-income countries, along with a staggering economic burden. We aimed to quantify the extent of OOP health expenditures and the magnitude of associated catastrophic and impoverishing health expenditures (CHE and IHE) for chronic KD (CKD) care in Ethiopia.
Methods: We conducted a prospective costing analysis for CKD care from the patient perspective. We collected data on OOP health expenditures (2023 US$) and household consumption expenditures from a cohort of 433 patients that were followed prospectively for 6 months. Patients were recruited from six health facilities from four constituencies in Ethiopia. We estimated the burden of OOP payments as the sum of direct medical expenditures (DMEs) and direct non-medical expenditures (DNMEs). DMEs were calculated by summing OOP payments for consultations, diagnostic workups, procedures, medications and hospital stays. DNMEs were computed by totalling OOP expenses for transportation, food and lodging. Additionally, we estimated the economic value of productivity losses incurred by patients and/or caregivers due to time spent seeking care. We used descriptive statistics to measure the extent of CHE and IHE. We ran a logistic regression model to assess the drivers of CHE.
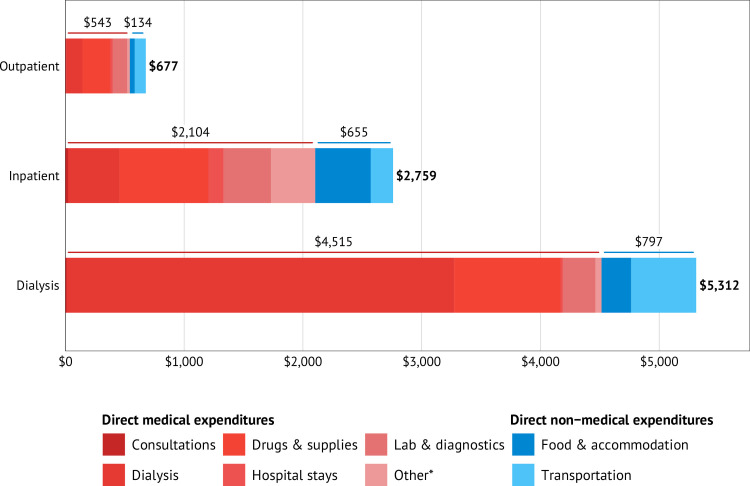
Results: The mean annual OOP expenditure was US$2337 (95% CI US$2014 to US$2659) and varied by type of care: US$677 (95% CI US$511 to US$825) for outpatient care, US$2759 (95% CI US$1171 to US$4347) for inpatient care and US$5312 (95% CI US$4644 to US$5919) for haemodialysis. DMEs (particularly haemodialysis) were the major drivers of cost, accounting for 76%-85% of the total OOP expenditure. Transportation expenditures were the major contributors among the DNMEs. Among those who sought outpatient, inpatient and haemodialysis care, 36%, 67% and 90% incurred CHE, respectively, at a 10% threshold of annual consumption expenditures. Among all patients, 25.6% of households were impoverished due to OOP medical expenditures, with the rate substantially higher among those requiring haemodialysis (43.4%). Facility type and the type of visit were significantly associated with the odds of incurring CHE (p<0.05), while adjusting for wealth quintile, disease stage, area of residence (urban/rural), family size, patient age and insurance membership status.
Conclusions: The household economic burden for CKD care is substantial, likely hindering access to necessary treatment and exacerbating the impoverishment, which is prevalent in Ethiopia. This would be an obstacle in achieving universal health coverage and Sustainable Development Goals in Ethiopia.
Keywords: Africa South of the Sahara; health economics.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Out-of-pocket expenditures and financial risks associated with treatment of vaccine-preventable diseases in Ethiopia: A cross-sectional costing analysis.PLoS Med. 2023 Mar 10;20(3):e1004198. doi: 10.1371/journal.pmed.1004198. eCollection 2023 Mar. PLoS Med. 2023. PMID: 36897870 Free PMC article.
-
Catastrophic out-of-pocket payments related to non-communicable disease multimorbidity and associated factors, evidence from a public referral hospital in Addis Ababa Ethiopia.BMC Health Serv Res. 2024 Aug 6;24(1):896. doi: 10.1186/s12913-024-11392-3. BMC Health Serv Res. 2024. PMID: 39107740 Free PMC article.
-
Determining household out of pocket payments, incidence of catastrophic expenditures and impoverishment among patients with malaria in Zambia's path towards Universal Health Coverage.PLoS One. 2024 Dec 10;19(12):e0312906. doi: 10.1371/journal.pone.0312906. eCollection 2024. PLoS One. 2024. PMID: 39656710 Free PMC article.
-
Economic Burden of Chronic Ill Health and Injuries for Households in Low- and Middle-Income Countries.In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R, editors. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 27. Chapter 6. In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R, editors. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 27. Chapter 6. PMID: 30212160 Free Books & Documents. Review.
-
Understanding variations in catastrophic health expenditure, its underlying determinants and impoverishment in Sub-Saharan African countries: a scoping review.Syst Rev. 2018 Sep 11;7(1):136. doi: 10.1186/s13643-018-0799-1. Syst Rev. 2018. PMID: 30205846 Free PMC article.
References
-
- Ferrari AJ, Santomauro DF, Aali A. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2133–61. doi: 10.1016/S0140-6736(24)00757-8. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous