

Real-time changes in pulse pressure during a 10-second end-expiratory occlusion test reliably detect preload responsiveness
- PMID: 40514683
- PMCID: PMC12166565
- DOI: 10.1186/s13054-025-05483-8
Real-time changes in pulse pressure during a 10-second end-expiratory occlusion test reliably detect preload responsiveness
Erratum in
-
Correction: Real-time changes in pulse pressure during a 10-second end-expiratory occlusion test reliably detect preload responsiveness.Crit Care. 2025 Aug 19;29(1):364. doi: 10.1186/s13054-025-05609-y. Crit Care. 2025. PMID: 40830885 Free PMC article. No abstract available.
Abstract
Background: The end-expiratory occlusion (EEO) test detects preload responsiveness through changes in cardiac index (ΔCI) during a 15-second respiratory hold at end-expiration. We investigated the diagnostic accuracy of EEO-induced changes in arterial pulse pressure (∆PP), especially when the duration of EEO is reduced to 10'' and 5'', and whether adding an end-inspiratory occlusion (EIO) improves this diagnostic accuracy.
Methods: In 143 mechanically ventilated patients with sinus rhythm, EEO and EIO were performed while recording ΔCI and ∆PP values. Either a fluid bolus-induced ΔCI ≥ 15% or a passive leg raising-induced ΔCI ≥ 10% defined preload responsiveness. The effects of the EEO and EIO tests on PP and CI were evaluated as the percentage difference between values averaged either over the last five seconds of the 15-sec respiratory holds (ΔPPEEO-15'' and ΔPPEIO-15'', ΔCIEEO-15'' and ΔCIEIO-15''), or between the 5th and the 10th seconds of the 15-sec respiratory holds (ΔPPEEO-10'' and ΔPPEIO-10'', ΔCIEEO-10'' and ΔCIEIO-10''), or during the five first seconds of respiratory holds (ΔPPEEO-5'' and ΔPPEIO-5'', ΔCIEEO-5'' and ΔCIEIO-5'') and baseline.
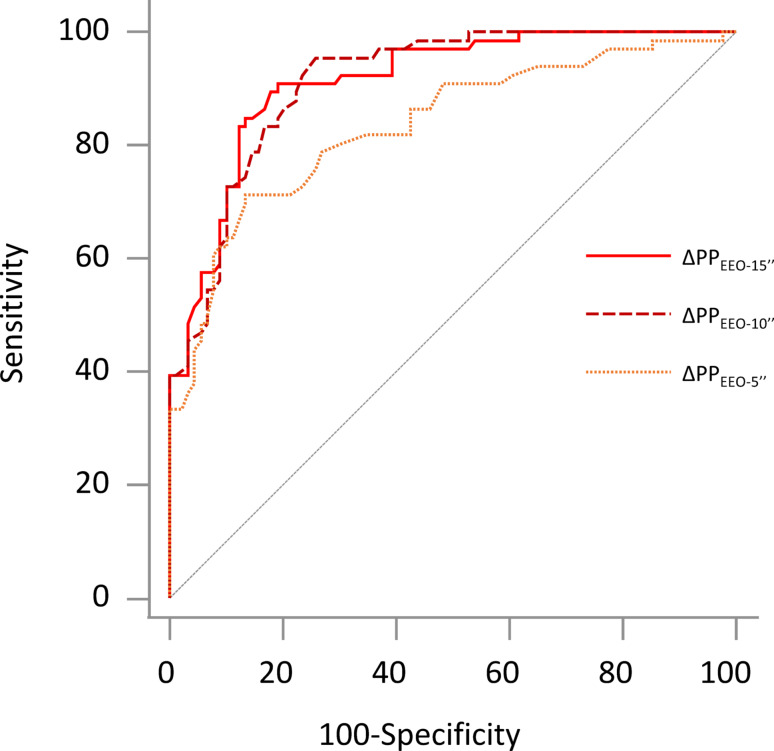
Results: Sixty-one (43%) patients were preload responders. Both ∆CIEEO-15'' and ∆CIEEO-10'' were higher in responders than in non-responders' (5.8 [4.5-7.3]% vs. 1.1 [0.1-3.4]% and 3.0 [2.4-4.3]% vs. 0.6 [0.1-1.6]%, respectively; p < 0.001), whereas ∆CIEEO-5'' did not differ between responders and non-responders. ∆PPEEO-5'', ∆PPEEO-10'' and ∆PPEEO-15'' were significantly higher in responders than in non-responders (5.2 [2.8-8.7]% vs. 1.2 [0.3-2.8]%, 7.7 [5.0-12.4]% vs. 1.8 [0.5-3.1]% and 8.1 [5.1-11.8]% vs. 1.5 [0.5-3.0]%, respectively; p < 0.001). For detecting preload responsiveness, compared to the area under the receiver operating characteristic (AUROC) of ∆CIEEO-15'' (0.935 [0.881-0.969]), the AUROC of ∆CIEEO-10'' was similar (0.910 [0.851-0.951], p = 0.410), but the AUROC of ∆CIEEO-5'' was smaller (0.541 [0.456-0.625], p < 0.001); the AUROC of ∆PPEEO-15'' (0.913 [0.857-0.952], p = 0.346), and ∆PPEEO-10'' (0.912 [0.860-0.947], p = 0.336) were similar, but the AUROC of ∆PPEEO-5'' (0.834 (0.763-0.891, p = 0.005) was significantly smaller. Evaluation of ∆CIEEO+EIO and ∆PPEEO+EIO did not enhance reliability of the test at each test duration.
Conclusion: In ventilated patients with sinus rhythm, real-time changes in PP during a 10-second EEO reliably detect preload responsiveness.
Trial registration: No. IDRCB 2010A0095942. Registered 04 January 2010.
Keywords: Cardiac output; Fluid challenge; Fluid responsiveness; Haemodynamic monitoring; Passive leg Raising.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Data collection of each study was approved by an independent ethics committee (Comité pour la Protection des Personnes, Ile-de-France VII). Informed consent was obtained from each patient or from the patient’s legally authorized representative if the patient was unable to provide consent. The study was conducted in accordance with the Declaration of Helsinki. Consent for publication: All authors of the manuscript have read and agreed to its content and are accountable for all aspects of the accuracy and integrity of the manuscript. The data were used anonymously. Competing interests: FG has no conflicts of interest to disclose.NDV has no conflict of interest to discloseCL has received fees for lectures from Sedana MedicalDA has no conflict of interest to discloseAP has no conflict of interest to discloseMJ has no conflict of interest to discloseSR has no conflict of interest to discloseIA has no conflict of interest to discloseAB has no conflict of interest to discloseJLT has received fees for lectures from Masimo and Edwards Lifesciences. He has received fees for consulting from Pulsion Medical Systems (Getinge).XM has received fees for lectures from Baxter Healthcare, Philips, Masimo, AOP and Pulsion Medical Systems (Getinge). He has received fees for consulting from Pulsion Medical Systems (Getinge).
Figures


References
-
- Biais M, Larghi M, Henriot J, de Courson H, Sesay M, Nouette-Gaulain K. End-Expiratory occlusion test predicts fluid responsiveness in patients with protective ventilation in the operating room. Anesth Analg. 2017;125:1889–95. - PubMed
-
- Messina A, Montagnini C, Cammarota G, De Rosa S, Giuliani F, Muratore L, et al. Tidal volume challenge to predict fluid responsiveness in the operating room: an observational study. Eur J Anaesthesiol. 2019;36:583–91. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
