

ATRX loss in adult gliomas lacking H3 alterations or IDH mutations, an exceptional situation for exceptional diagnoses: the experience of Sainte-Anne hospital
- PMID: 40514723
- PMCID: PMC12164129
- DOI: 10.1186/s40478-025-02044-6
ATRX loss in adult gliomas lacking H3 alterations or IDH mutations, an exceptional situation for exceptional diagnoses: the experience of Sainte-Anne hospital
Abstract
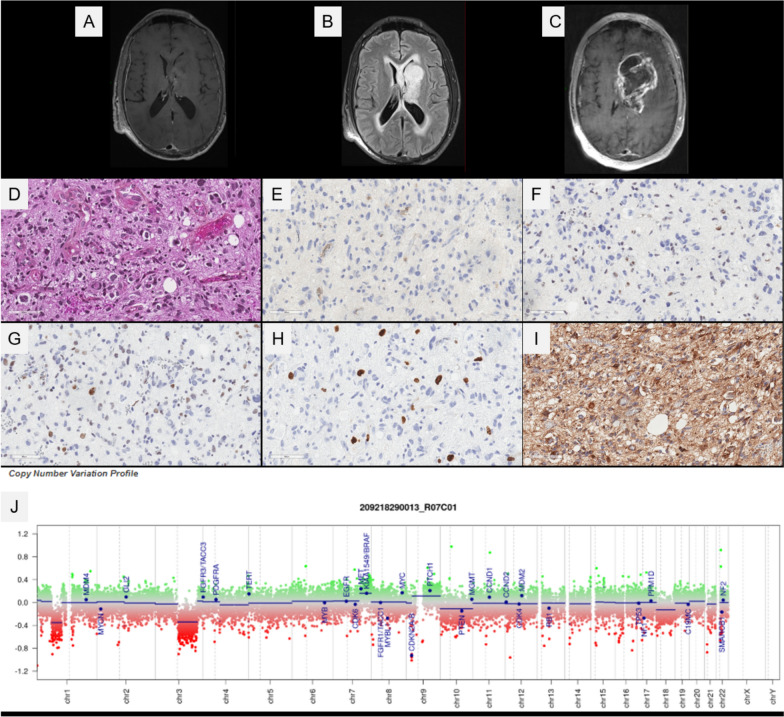
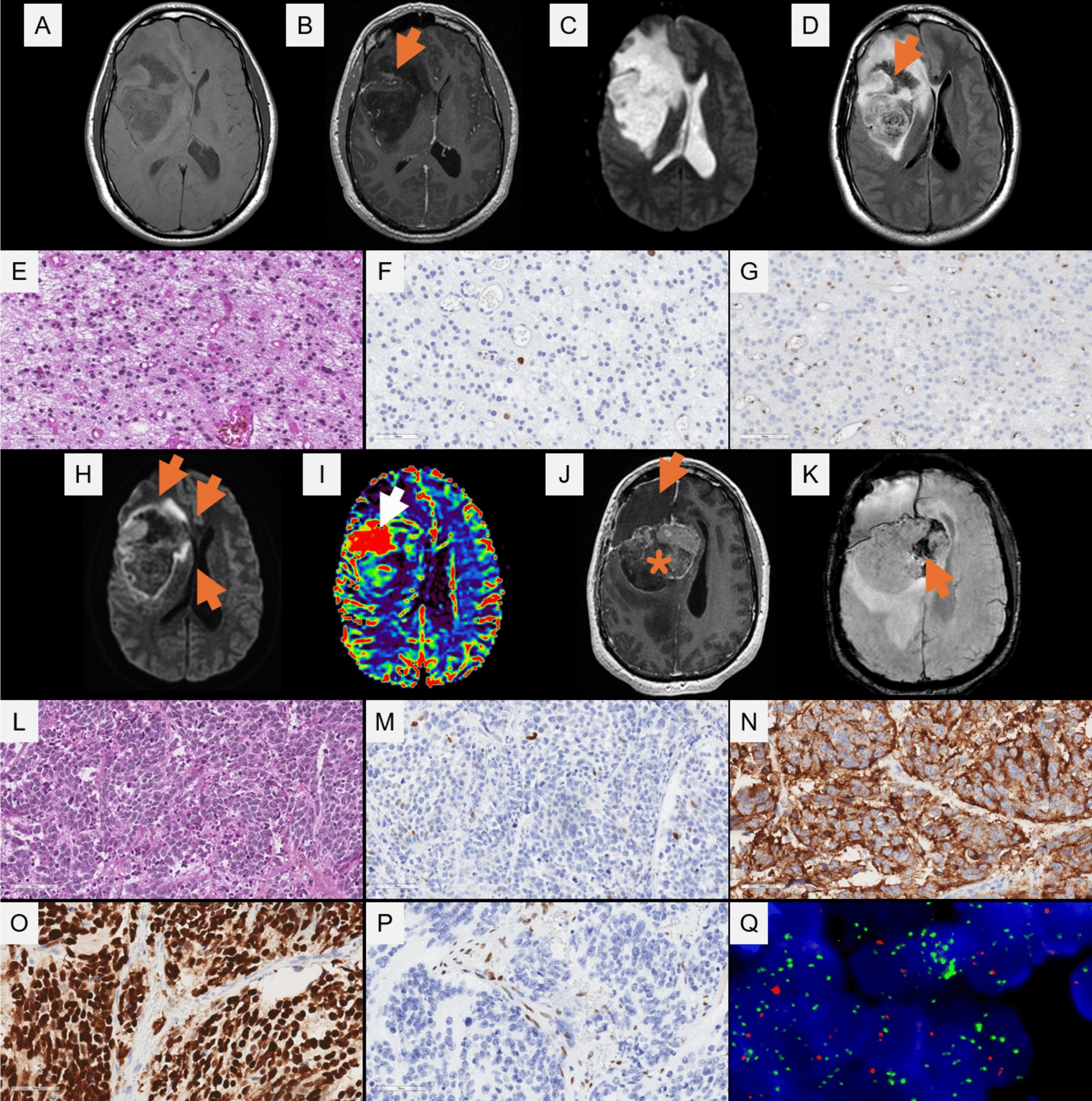
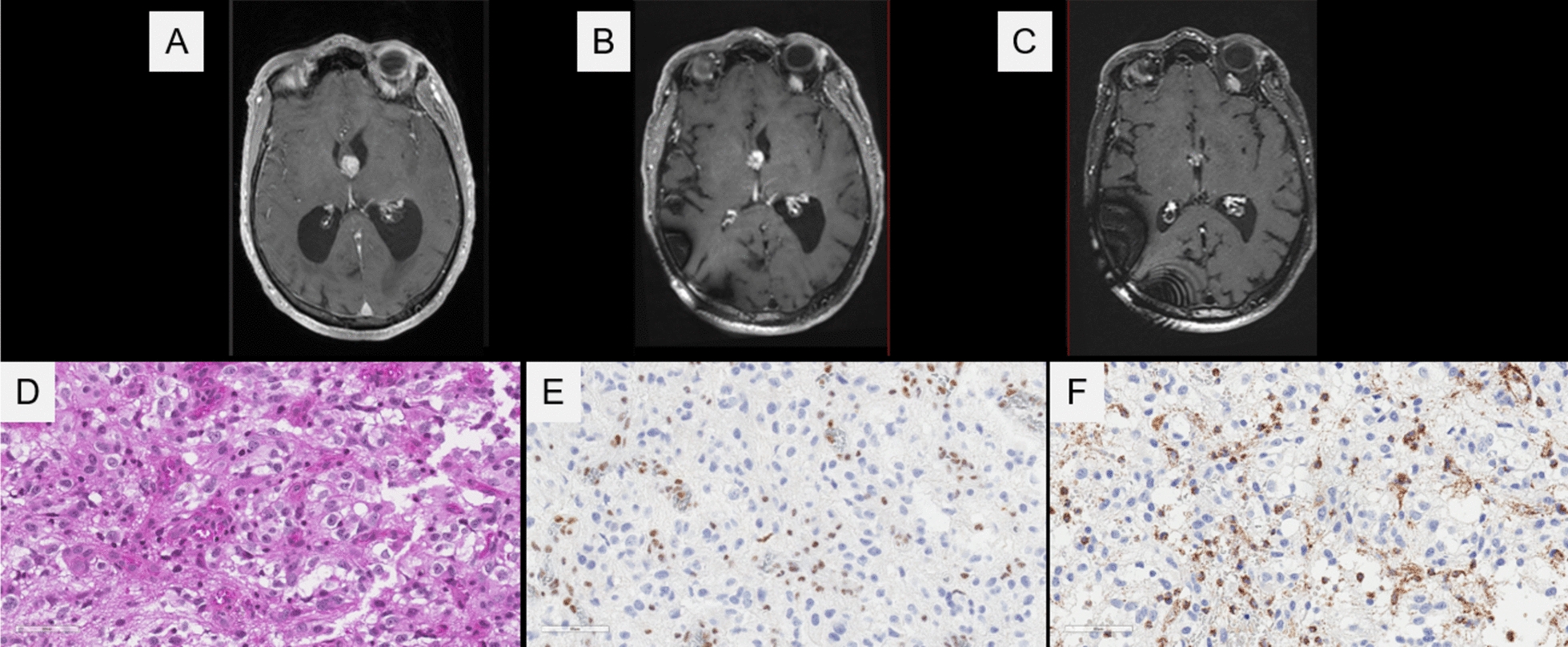
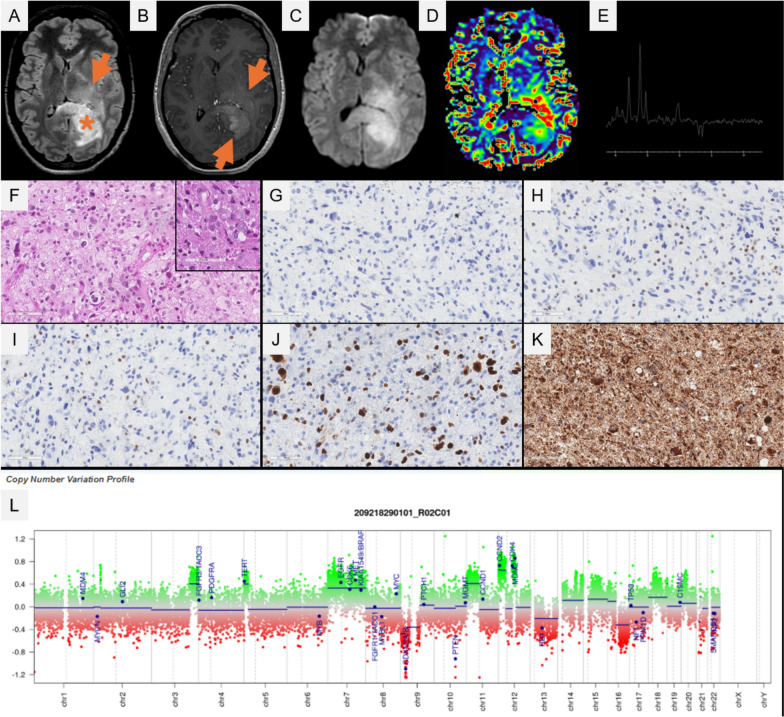
ATRX immunostaining constitutes a routinely used biomarker for the practice of neuropathology. The loss of ATRX expression correlating with ATRX gene alterations is implicated in a wide variety of pediatric and adult gliomas, and has been indexed as a desirable or essential diagnostic criterion for four tumor types featured in the latest world health organization classification of central nervous system Tumors. In adult-type diffuse glioma, the loss of ATRX expression is a hallmark of astrocytoma, IDH-mutant. Recently, novel tumor types and alterations have been referenced in the literature. These include the high-grade astrocytoma with piloid features (HGAP), for which no consistent clinicopathological features have been defined, and the presence of other alterations in the Krebs cycle genes (variants of the Fumarate hydratase -FH- gene) found in gliomas resembling astrocytomas, IDH-mutant. Because of this rapidly evolving classification and histomolecular landscape, we retrospectively analyzed adult gliomas diagnosed over a four consecutive year period to identify supratentorial gliomas, lacking H3 alterations or IDH mutations and harboring a loss of ATRX expression, in order to update their diagnoses in terms of histopathology, genetics and epigenetics. Four specimens (from 620 adult gliomas, 0.7%) were reclassified at the end of the molecular workup, as: 1/ one HGAP, 2/ one malignant transformation with a primitive neuronal component of an astrocytoma, IDH-mutant which lost the IDH2 mutation at recurrence, 3/ a glioma, FH-mutant for which the histopathological and epigenetic features were similar to an astrocytoma, IDH-mutant, and 4/ a glioblastoma, IDH-wildtype. To conclude, these exceptional cases extend the spectrum of ATRX loss in gliomas, beyond the astrocytoma, IDH-mutant and the diffuse hemispheric glioma, H3 G34-mutant.
Keywords: ATRX; Diffuse glioma; FH; HGAP.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by GHU Paris Psychiatry and Neurosciences, Sainte-Anne Hospital’s local ethic committee. Consent for publication: The patient signed informed consent forms before treatment was started. Competing interests: The authors declare that they have no conflicts of interest directly related to the topic of this article.
Figures
References
-
- Reuss DE, Sahm F, Schrimpf D, Wiestler B, Capper D, Koelsche C et al (2015) ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an “integrated” diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. Acta Neuropathol (Berl) 129(1):133–146 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
