

Beyond overweight, visceral adiposity is associated with estimation of cardiovascular risk in patients living with type 1 diabetes: findings from the SFDT1 cohort
- PMID: 40517273
- PMCID: PMC12166620
- DOI: 10.1186/s12933-025-02789-3
Beyond overweight, visceral adiposity is associated with estimation of cardiovascular risk in patients living with type 1 diabetes: findings from the SFDT1 cohort
Abstract
Introduction & objectives: As in the general population, people living with type 1 diabetes (PWT1D) are faced with overweight and obesity, which contribute to cardiovascular (CV) risk. However, the role of visceral adiposity, due to its adverse metabolic profile, should also be addressed in PWT1D. We aimed to assess the 10-year CV risk of PWT1D according to body mass index (BMI) and waist-to-height ratio (WHtR), a parameter for estimating visceral adiposity.
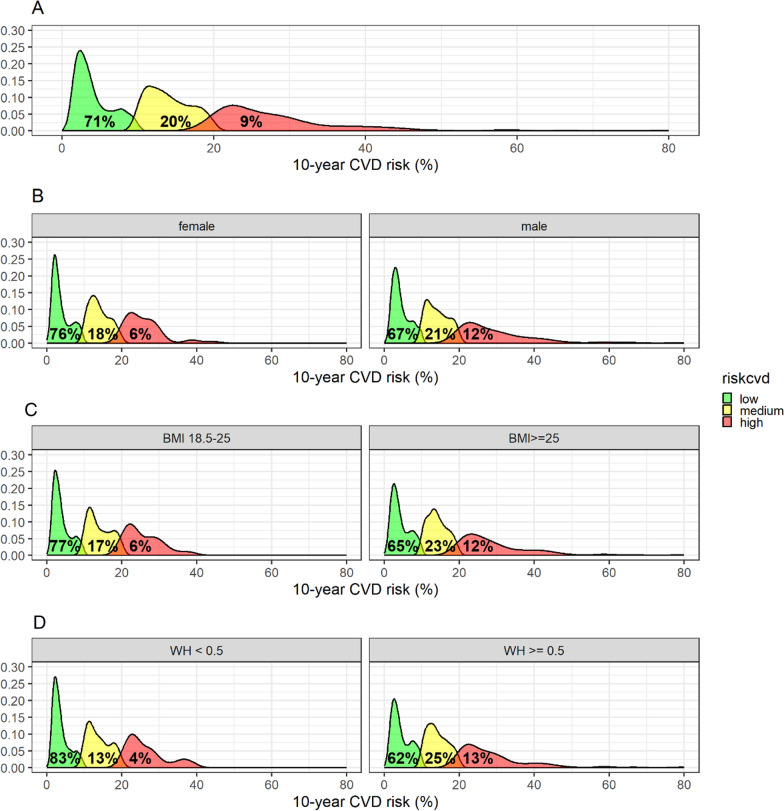
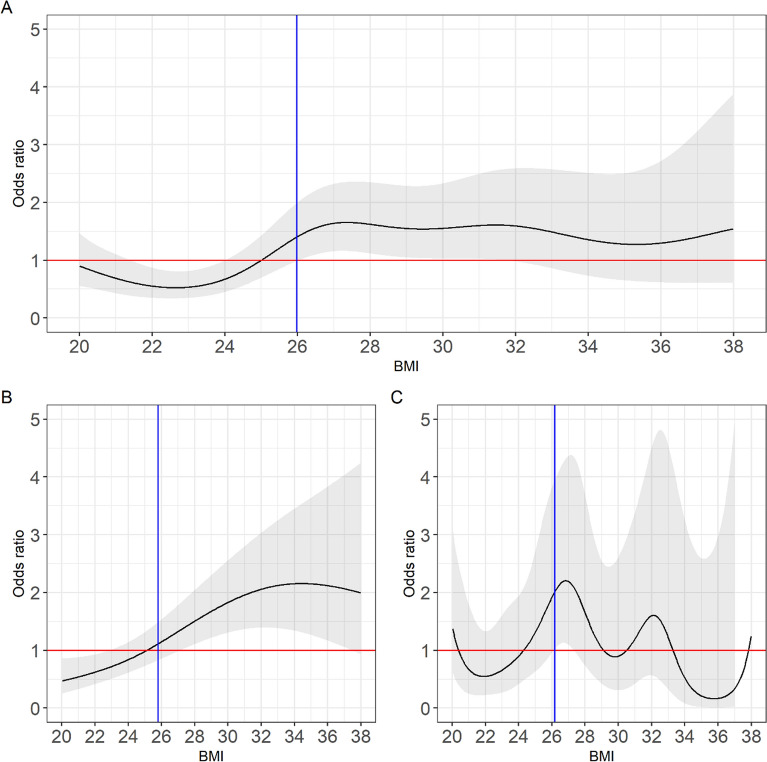
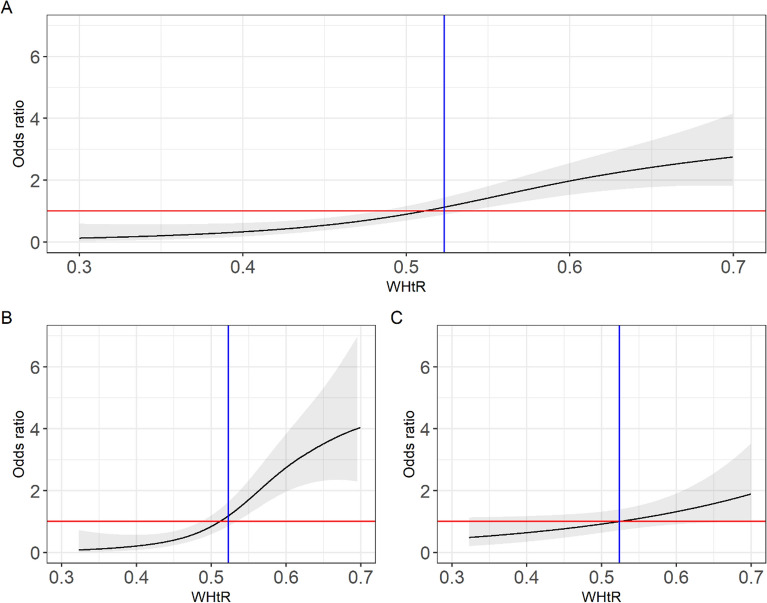
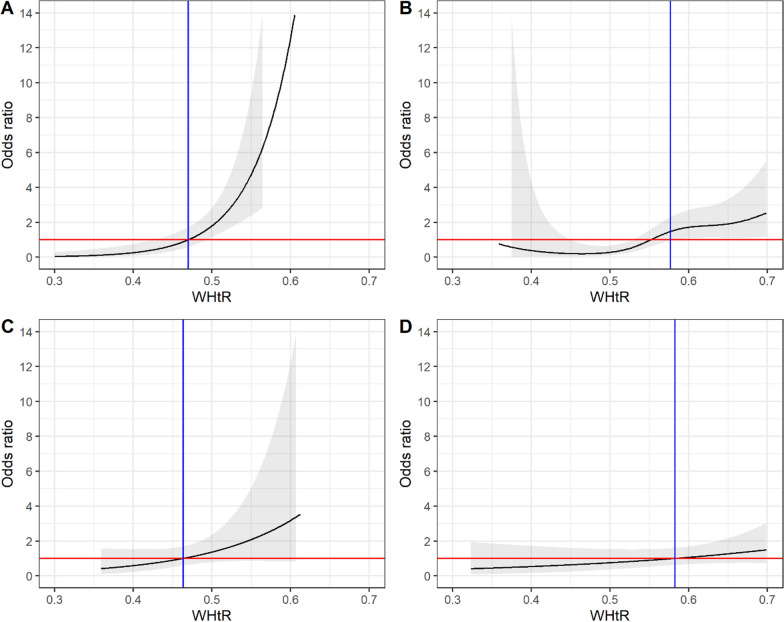
Methods: In this cross-sectional study, PWT1D in primary CV prevention from the SFDT1 cohort were categorized by BMI status, either normal (18.5-24.9 kg/m2) or overweight/obesity (≥ 25 kg/m2), and by WHtR according to the validated threshold of 0.5. The 10-year CV risk was estimated using the Steno Type 1 Risk Engine and classified into three categories: low (< 10%), intermediate (10-20%) and high (> 20%). The distribution of CV risk was assessed using density plots. In multivariable analysis, the association between BMI, WHtR, and high estimated 10-year CV risk was studied using spline regression models with sex stratification. Thresholds were determined by the Receiver Operating Characteristic (ROC) curve.
Results: The study included 1,482 patients; 49.9% had a normal BMI, and 50.1% a BMI ≥ 25 kg/m2. The proportion of patients with high CV risk was higher in PWT1D with overweight/obesity (12% vs. 7%) and in those with WHtR ≥ 0.5 (13% vs. 4%). BMI was significantly associated with high CV risk in men (p = 0.001) but a non-significant trend was found in women (p = 0.053). WHtR was significantly associated with high CV risk in both men (p < 0.001) and women (p = 0.046). The BMI threshold associated with high CV risk was 24.9 kg/m2 for men, and the WHtR threshold was 0.5 for both men and women.
Conclusion: In PWT1D in condition of primary CV prevention, visceral adiposity, assessed by WHtR, is a more robust marker of estimated 10-year CV risk than overweight/obesity status in both men and women.
Keywords: Adiposity distribution; Body mass index; Cardiovascular risk; Registry; Sex; Type 1 diabetes; Waist circumference.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: SFDT1 was approved by an ethical committee on 5 November 2019 and is declared in clinical trial NCT04657783. Consent for publication: Not applicable. Competing interests: EBP reports receiving lecture honorariums from Astra Zeneca and Sanofi, and has been an employee of Boehringer Ingelheim since February 2024. The other authors declare that they have no competing interests.
Figures
References
-
- Rawshani A, Rawshani A, Franzén S, Eliasson B, Svensson A-M, Miftaraj M, et al. Mortality and cardiovascular disease in type 1 and Type 2 Diabetes. N Engl J Med. 2017;376:1407–18. - PubMed
-
- Lind M, Svensson A-M, Kosiborod M, Gudbjörnsdottir S, Pivodic A, Wedel H, et al. Glycemic control and excess mortality in type 1 diabetes. N Engl J Med. 2014;371:1972–82. - PubMed
-
- Lavens A, Nobels F, De Block C, Oriot P, Verhaegen A, Chao S, et al. Effect of an integrated, multidisciplinary nationwide approach to type 1 diabetes care on metabolic outcomes: an observational real-world study. Diabetes Technol Ther. 2021;23:565–76. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
