

Comparative risk of severe constipation in patients treated with opioids for non-cancer pain: a retrospective cohort study in Northwest England
- PMID: 40518524
- PMCID: PMC12168406
- DOI: 10.1186/s12916-025-04118-7
Comparative risk of severe constipation in patients treated with opioids for non-cancer pain: a retrospective cohort study in Northwest England
Abstract
Background: Constipation is a frequent adverse event associated with opioid medications that can have a considerable impact on patients' quality of life. In patients who require opioids for pain relief, less is known about the risk conferred by specific opioids given their diverse pharmacology and the effect of daily dose and potency. The aim of the study was to evaluate the comparative risk of severe constipation by opioid type and dose in patients with non-cancer pain admitted to hospital.
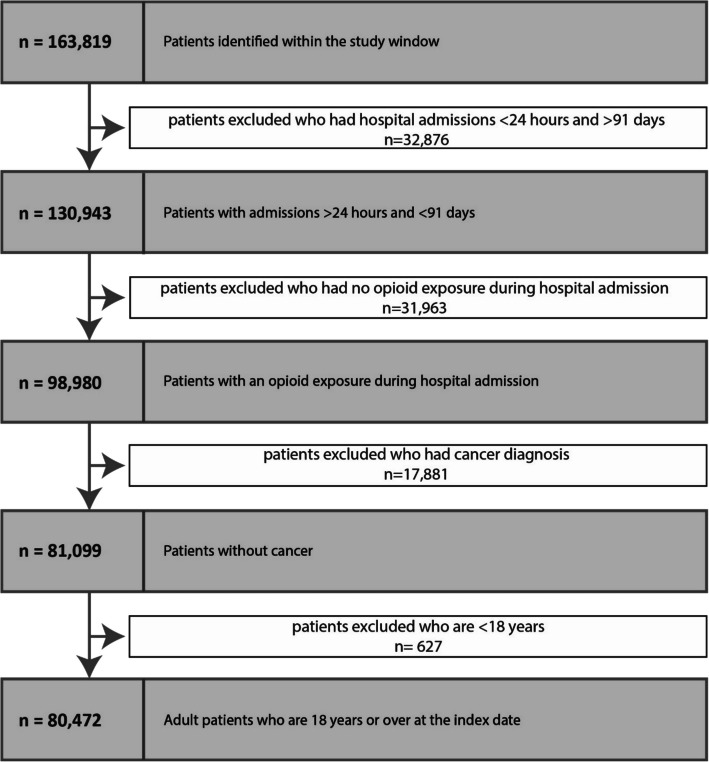
Methods: We conducted a retrospective cohort study using hospital electronic health records in Northwest England between December 1, 2009, and December 31, 2020. Patients who were ≥ 18 years and without a history of cancer were included. Opioid exposure was measured using administered drug information in hospital. The outcome was a severe constipation event defined as administration of an enema or suppository. Incidence rates by opioid use status, type of opioid class and morphine milligram equivalent (MME) per day were calculated, and a Cox regression model was used to determine associations with incident constipation after adjusting for confounders.
Results: The study included 80,475 eligible patients who were administered an opioid in hospital. Compared to codeine, morphine (HR 1.59, 95% CI 1.45-1.74), oxycodone (HR 1.46, 95% CI 1.32-1.63), fentanyl (HR 1.37, 95% CI 1.14-1.64) and combination opioids (HR 1.85, 95% CI 1.66-2.06) were associated with a higher risk of constipation in the fully adjusted models. Tramadol demonstrated a significantly lower risk compared to codeine (HR 0.80, 95% CI 0.64-1.00). Higher opioid doses of more than ≥ 50 MME/day in comparison to < 50 MME/day were associated with an increased risk of constipation (compared to < 50 MME/day, 50 to < 120 MME/day: HR 1.95, 95% CI 1.78-2.15; ≥ 120 MME/day: HR 1.45, 95% CI 1.32-1.60).
Conclusions: Morphine, oxycodone, fentanyl and combination opioids administration were associated with a significantly higher risk of severe constipation compared to codeine. Tramadol was associated with the lowest risk of the outcome compared to codeine. Patients on ≥ 50 MME/day experienced a higher risk of severe constipation compared to those on < 50 MME/day. These results can be used to guide better shared decisions with patients to balance benefit and harms of specific opioid types and doses.
Keywords: Adverse events; Chronic pain; Constipation; Drug safety; Electronic health records; Morphine milligram equivalents; Opiates; Opioid-related harms; Opioids.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study received ethics approval from the Health Research Authority (Reference 21/EM/0147; East Midlands Leicester South) and was performed in accordance with the Declaration of Helsinki. No patient identifiable information was accessible to the researchers. As this study used pseudonymised data only, individual written consent of each patient was not necessary as per the HRA approvals. Consent for publication: All authors consent for publication. Competing interests: The authors declare no competing interests.
Figures
References
-
- Kalkman GA, Kramers C, van Dongen RT, van den Brink W, Schellekens A. Trends in use and misuse of opioids in the Netherlands: a retrospective, multi-source database study. Lancet Public Heal. 2019;2667. 10.1016/S2468-2667(19)30128-8. - PubMed
-
- Els C, Jackson TD, Kunyk D, Lappi VG, Sonnenberg B, Hagtvedt R, et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of Cochrane Reviews. Cochrane Database of Systematic Reviews. John Wiley and Sons Ltd; 2017. 10.1002/14651858.CD012509.pub2. - PMC - PubMed
-
- Huang Y, Mccarthy C, Jani M. Balancing the evidence: an update on analgesic use in rheumatic and musculoskeletal diseases. Front Drug Saf Regul. 2023; 1–13. 10.3389/fdsfr.2023.1117674.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
