

Risk-adapted intensification therapy in high-risk prostate cancer: how relevant is the role of radiation dose
- PMID: 40518535
- PMCID: PMC12167573
- DOI: 10.1186/s13014-025-02665-0
Risk-adapted intensification therapy in high-risk prostate cancer: how relevant is the role of radiation dose
Abstract
Background/purpose: Dose escalation has demonstrated a significant improvement in biochemical recurrence in high-risk prostate cancer (HRPCa). We evaluated the impact on overall survival (OS) of dose intensification with external beam radiation therapy (EBRT) in a cohort of HRPCa patients treated in a single institution.
Methods and materials: Between January 1997 and January 2024, a total of 1451 consecutive localized PCa patients were treated with primary EBRT alone as part of a prospective institutional program for risk-adapted dose-intensification radiotherapy. For the present analysis, we specifically selected a cohort of 424 consecutive HRPCa patients with a minimum follow-up (FU) of 5 years. The median RT dose was 79.2 Gy (interquartile range [IQR] 74.9-80.3). Short and long-term hormones were administered in 56 (13%) and 350 (83%) of patients respectively. Kaplan-Meier curves were used to calculate overall survival (OS). Cumulative incidence of distant metastasis (DM), and cause specific survival (CSS) were estimated using competing risk regression.
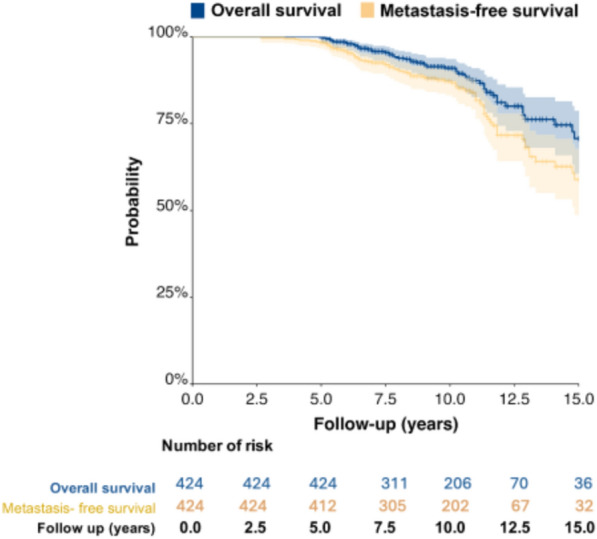
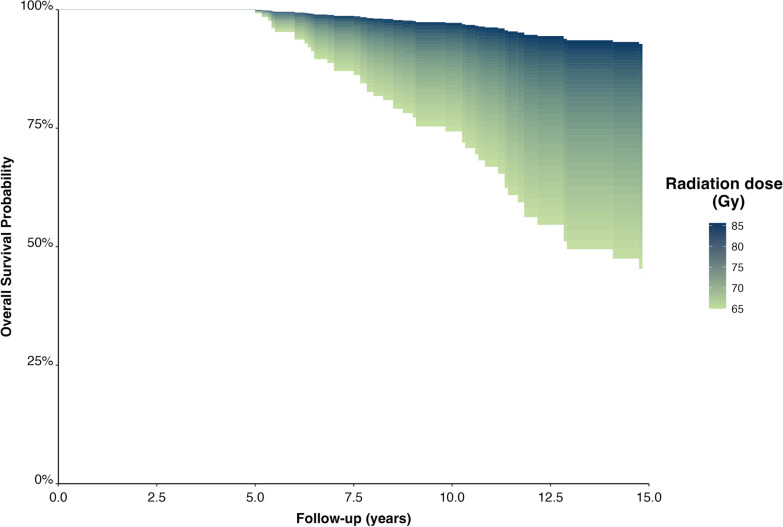
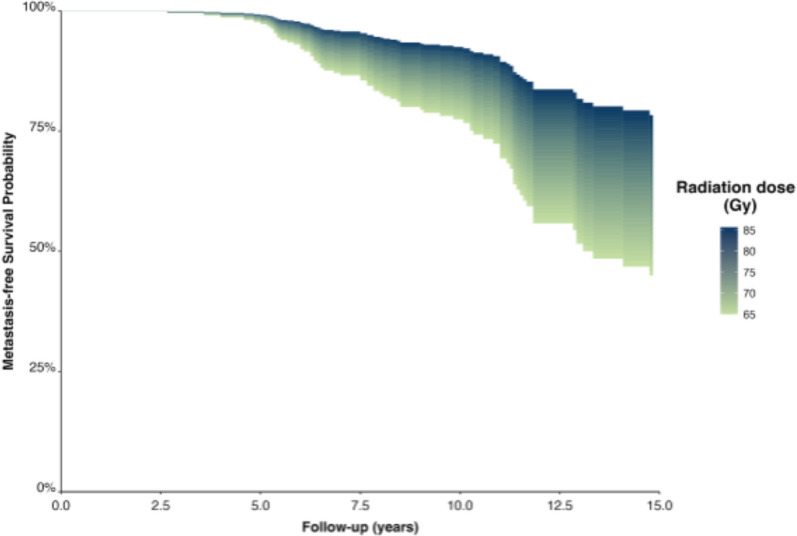
Results: Median patient age was 69 years (IQR 65-72) and median FU was 118 months (IQR 88.0-135.0). At the time of analysis, 54 of 424 patients (13%) had died. The leading cause of death was cardiovascular disease in 16/54 patients (4%), followed by PCa in 15 patients (3%). At 10 and 15 years, the KM estimated OS rates were 91% (95% CI 87-93) and 71% (95% CI 61-79), respectively. The corresponding rates for MFS were 87% (95% CI 83-90) and 60% (95% CI 49-68), and for CSS were 97% (95% CI 95-99) and 90% (95% CI 49-81), respectively. In multivariate analysis, when adjusted for patient age, T stage, Gleason/ISUP group, PSA and length of hormone-therapy, higher radiation dose remained significantly associated with an improved OS (HR 0.89; 95% CI 0.84-0.94), MFS (HR 0.94; 95% CI 0.90-0.98) and CSS (HR 0.89; 95% CI 0.84-0.94).
Conclusions: The present study confirms that radiation dose intensification is paramount in the treatment of HRPCa with independence of duration of ADT.
Keywords: Androgen deprivation; High-risk prostate cancer; Metastasis-free survival; Overall survival; Radiation dose escalation; Radiotherapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. This is retrospective analysis of a prospective cohort, not a clinical trial. But, all patients signed an ICF prior to radiation therapy as clinical practice in all cases. Consent for publication: Not applicable. The clinical research of the present manuscripts comply with international and national standards for such work (such as the Declaration of Helsinki ) Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
The need for androgen deprivation therapy in patients with intermediate-risk prostate cancer treated with dose-escalated external beam radiation therapy.Can J Urol. 2017 Feb;24(1):8656-8662. Can J Urol. 2017. PMID: 28263132
-
Dose escalation for prostate cancer radiotherapy: predictors of long-term biochemical tumor control and distant metastases-free survival outcomes.Eur Urol. 2011 Dec;60(6):1133-9. doi: 10.1016/j.eururo.2011.08.029. Epub 2011 Aug 22. Eur Urol. 2011. PMID: 21889832 Free PMC article.
-
Short-term androgen-deprivation therapy improves prostate cancer-specific mortality in intermediate-risk prostate cancer patients undergoing dose-escalated external beam radiation therapy.Int J Radiat Oncol Biol Phys. 2013 Mar 15;85(4):1012-7. doi: 10.1016/j.ijrobp.2012.07.2374. Epub 2012 Sep 14. Int J Radiat Oncol Biol Phys. 2013. PMID: 22981709
-
Outcomes and prognostic factors in intermediate-risk prostate cancer: multi-institutional analysis of the Spanish RECAP database.Clin Transl Oncol. 2019 Jul;21(7):900-909. doi: 10.1007/s12094-018-02000-y. Epub 2018 Dec 10. Clin Transl Oncol. 2019. PMID: 30536208
-
Benefits and Risks of Primary Treatments for High-risk Localized and Locally Advanced Prostate Cancer: An International Multidisciplinary Systematic Review.Eur Urol. 2020 May;77(5):614-627. doi: 10.1016/j.eururo.2020.01.033. Epub 2020 Mar 4. Eur Urol. 2020. PMID: 32146018
References
-
- Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Brunckhorst O, Darraugh J, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024 Update. Part I: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2024;86(2):148–63. 10.1016/j.eururo.2024.03.027. - PubMed
-
- Heemsbergen WD, Al-Mamgani A, Slot A, Dielwart MF, Lebesque JV. Long-term results of the Dutch randomized prostate cancer trial: impact of dose-escalation on local, biochemical, clinical failure, and survival. Radiother Oncol. 2014;110:104–9. - PubMed
-
- Beckendorf V, Guerif S, Le Prisé E, et al. 70 Gy versus 80 Gy in localized prostate cancer: 5-year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys. 2011;80(4):1056–63. - PubMed
-
- Dearnaley DP, Jovic G, Syndikus I, et al. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: long-term results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2014;15(4):464–73. - PubMed
-
- Morris WJ, Tyldesley S, Rodda S, et al. Androgen suppression combined with elective nodal and dose escalated radiationtherapy (the ASCENDE-RT trial): an analysis of survival endpoints for a randomized trial comparing a low-dose-rate brachytherapy boost to a dose-escalated external beam boost for high- and intermediate-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2017;98:275–85. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
