

Voltage-Gradient Mapping-Guided Slow Pathway Ablation in Typical Atrioventricular Nodal Re-Entrant Tachycardia
- PMID: 40518701
- PMCID: PMC12266630
- DOI: 10.1111/pace.15223
Voltage-Gradient Mapping-Guided Slow Pathway Ablation in Typical Atrioventricular Nodal Re-Entrant Tachycardia
Abstract
Introduction: High-density mapping is useful for common atrioventricular nodal re-entrant tachycardia (AVNRT) ablation. This study aimed to evaluate the effective targets for slow pathway (SP) ablation using voltage-gradient mapping.
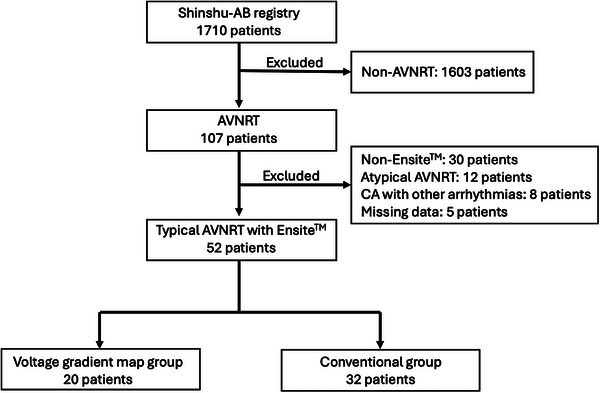
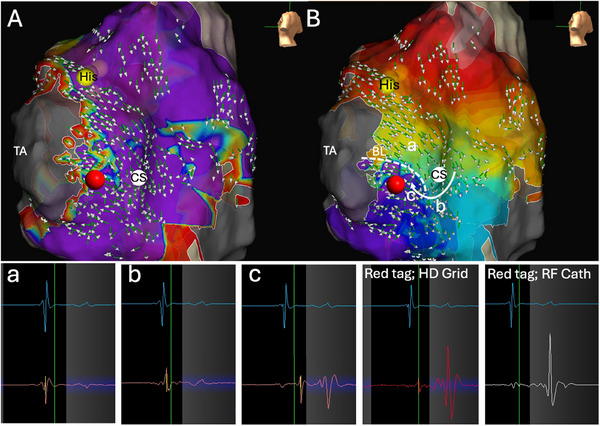
Methods: Fifty-two patients diagnosed with slow/fast AVNRT were enrolled. Patients underwent SP ablation using either a voltage-gradient map (n = 20) or a conventional approach based on anatomic and electrophysiological findings (n = 32). The Ensite X EP system was used as the 3-D mapping system in all patients. The target CA site was defined as the location at which the Jackman potential, with a voltage of <0.5 mV on the tricuspid annulus (TA) side of the pivot point, was confirmed by the creation of a voltage-gradient map with the Advisor HD Grid SE.
Results: The distance from the successful ablation site to the His bundle was significantly greater in the voltage-gradient map group (15.0 (12.8-19.0) vs. 11.0 (8.0-13.0) mm, p < 0.001), the junctional rhythm heart rate was slower (92.5 (78.8-121.8) vs. 114.0 (96.8-131.0) bpm, p = 0.028), and the time to the appearance of junctional rhythm after radiofrequency application was shorter (4.0 (2.5-7.3) vs. 7.8 (6.6-8.6) s, p = 0.002). Furthermore, the procedure time was also significantly shorter (53.5 (47.0-67.0) vs. 99.5 (76.3-112.5) min, p < 0.001) in the voltage-gradient map group.
Conclusion: The site at which the Jackman potential was confirmed, with a voltage of <0.5 mV on the TA side from the pivot point drawn using the voltage-gradient map, may be defined as the CA target of SP.
Keywords: 3‐D mapping; Advisor HD Grid mapping catheter; pivot point; slow pathway ablation; typical AVNRT; voltage‐gradient map.
© 2025 The Author(s). Pacing and Clinical Electrophysiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Unexpected transient atrioventricular block and slow junctional rhythm using pulsed field ablation for slow pathway modification: Excited or cautious for ablators.Heart Rhythm. 2025 Jul;22(7):1682-1692. doi: 10.1016/j.hrthm.2024.09.023. Epub 2024 Sep 19. Heart Rhythm. 2025. PMID: 39304002
-
Paradigm Shift for Catheter Ablation of Atypical Atrioventricular Nodal Re-Entrant Tachycardia: 3-Dimensional Mapping-Based Ablation.JACC Clin Electrophysiol. 2023 Aug;9(8 Pt 3):1730-1740. doi: 10.1016/j.jacep.2023.04.028. Epub 2023 Jun 21. JACC Clin Electrophysiol. 2023. PMID: 37354187
-
Comparative utility of omnipolar and bipolar electroanatomic mapping methods to detect and localize dual nodal substrate in patients with atrioventricular nodal reentrant tachycardia.J Interv Card Electrophysiol. 2024 Oct;67(7):1579-1591. doi: 10.1007/s10840-024-01800-3. Epub 2024 Apr 18. J Interv Card Electrophysiol. 2024. PMID: 38634991 Free PMC article.
-
Remote magnetic navigation for catheter ablation of atrioventricular nodal reentrant tachycardia: a systematic review and meta-analysis.Expert Rev Cardiovasc Ther. 2013 Jul;11(7):829-36. doi: 10.1586/14779072.2013.811968. Expert Rev Cardiovasc Ther. 2013. PMID: 23895026
-
Cryoablation versus radiofrequency ablation of atrioventricular nodal reentrant tachycardia.J Interv Card Electrophysiol. 2014 Mar;39(2):111-9. doi: 10.1007/s10840-013-9842-2. Epub 2013 Nov 29. J Interv Card Electrophysiol. 2014. PMID: 24293174
References
-
- Asirvatham S. J. and Stevenson W. G., “Atrioventricular Nodal Block With Atrioventricular Nodal Reentrant Tachycardia Ablation,” Circulation 8 (2015): 745–747. - PubMed
-
- Bailin S. J., Rhodes T., Arter C., Kocherla C., and Kaushik N., “Physiology of Slow Pathway Conduction During Sinus Rhythm: Evidence From High Density Mapping Within the Triangle of Koch,” Journal of Interventional Cardiac Electrophysiology 63 (2022): 573–580. - PubMed
-
- Kumagai K. and Toyama H., “Activation Pattern Within Koch's Triangle During Sinus Rhythm in Patients With and Without Atrioventricular Nodal Reentrant Tachycardia,” Journal of Interventional Cardiac Electrophysiology 67 (2024): 139–146. - PubMed
-
- Takahashi M., Yamaoka K., Kujiraoka H., Arai T., Hojo R., and Fukamizu S., “Peak Frequency Annotation Algorithm Guided Slow Pathway Ablation in Typical Atrioventricular Nodal Re‐Entrant Tachycardia,” Heart Rhythm 21 (2024): 2206–2214. - PubMed
-
- Katritsis D. G. and Josephson M. E., “Differential Diagnosis of Regular, Narrow QRS Tachycardias,” Heart Rhythm 12 (2015): 1667–1676. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
