

Application of New Pediatric Sepsis Definition to a Multicenter Observational Cohort of Previously Enrolled Severe Sepsis Patients Defined by SIRS Plus Organ Dysfunction
- PMID: 40518943
- PMCID: PMC12216587
- DOI: 10.1177/08850666251349790
Application of New Pediatric Sepsis Definition to a Multicenter Observational Cohort of Previously Enrolled Severe Sepsis Patients Defined by SIRS Plus Organ Dysfunction
Abstract
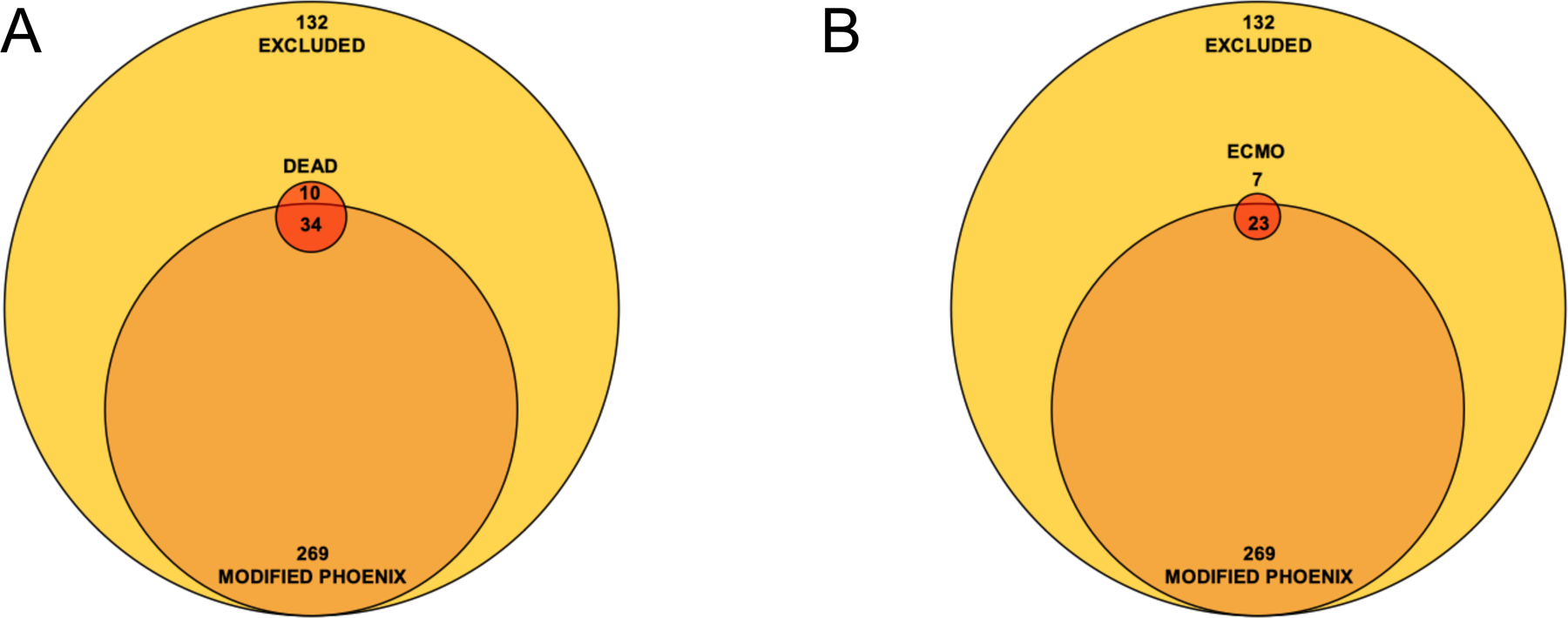
IntroductionIn 2024, a Society of Critical Care Medicine task force updated the pediatric sepsis definition from the presence of suspected or confirmed infection, and a systemic inflammatory response (SIRS) with organ dysfunction, to a novel definition. Our objective is to identify how many patients previously identified as having severe sepsis would continue to meet the new definition.Materials and methodsWe performed a secondary analysis of the Phenotyping Sepsis-Induced Multiple Organ Failure cohort of 401 children with suspected or confirmed infection, two of four SIRS criteria and organ dysfunction enrolled between 2015-2017. We calculated a modified Phoenix Sepsis Criteria Score (mPSC) for participants and compared those with mPSC of greater than or equal to 2 or less than 2 according to the 2024 definition.ResultsOf 401 children, 132 (33%) did not meet mPSC definitions. While children meeting mPSC had more organ dysfunction, the total mortality did not differ. One in 4 children requiring extracorporeal membrane oxygenation and 1 in 4 mortalities did not meet the mPSC definition. In logistic regression models, in the complete cohort, hematologic (OR 4.4, 95% CI: 1.8-10.2, P-value = .001), central nervous system (OR 2.3, 95% CI: 1.0-5.1, P-value = .046) and renal failure (OR: 3.2, 95% CI:1.2-7.9, P-value = .017) predicted mortality; in the mPSC subgroup pulmonary (OR: 3.6, 95% CI:1.3-13.3, P-value = .030) and hematologic failure (OR 5.6, 95% CI: 2.2-14.5, P-value = .0003) were significant predictors. In the mPSC excluded subgroup, only renal failure predicted mortality (OR 9.6, 95% CI 1.1-73.0, P-value = .028).ConclusionsFurther study of the impact of the 2024 data-driven organ dysfunction definition on pediatric sepsis research, patient safety, and clinical benchmarking efforts is warranted.
Keywords: infection; mortality; organ failure; pediatric sepsis; phoenix sepsis criteria; sepsis definitions.
Conflict of interest statement
Declaration of conflicting interest: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).JAMA. 2016 Feb 23;315(8):775-87. doi: 10.1001/jama.2016.0289. JAMA. 2016. PMID: 26903336 Free PMC article.
-
Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD012404. doi: 10.1002/14651858.CD012404.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938790 Free PMC article.
-
Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2017 May 23;5(5):CD011425. doi: 10.1002/14651858.CD011425.pub2. Cochrane Database Syst Rev. 2017. PMID: 28535331 Free PMC article.
-
Antithrombin III for critically ill patients.Cochrane Database Syst Rev. 2016 Feb 8;2(2):CD005370. doi: 10.1002/14651858.CD005370.pub3. Cochrane Database Syst Rev. 2016. PMID: 26858174 Free PMC article.
References
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–1655. doi: 10.1378/CHEST.101.6.1644 - DOI - PubMed
Grants and funding
- U10 HD050012/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- L30 AI147146/AI/NIAID NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- R01 GM108618/GM/NIGMS NIH HHS/United States
- U10 HD063108/HD/NICHD NIH HHS/United States
- K23 GM148827/GM/NIGMS NIH HHS/United States
- K23 HD099331/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
