

The Impact of Age and Gender on Cervical Vestibular-Evoked Myogenic Potentials Using 500 Hz Tone Bursts Stimuli: A Cross-Sectional Study
- PMID: 40519411
- PMCID: PMC12166493
- DOI: 10.7759/cureus.84142
The Impact of Age and Gender on Cervical Vestibular-Evoked Myogenic Potentials Using 500 Hz Tone Bursts Stimuli: A Cross-Sectional Study
Abstract
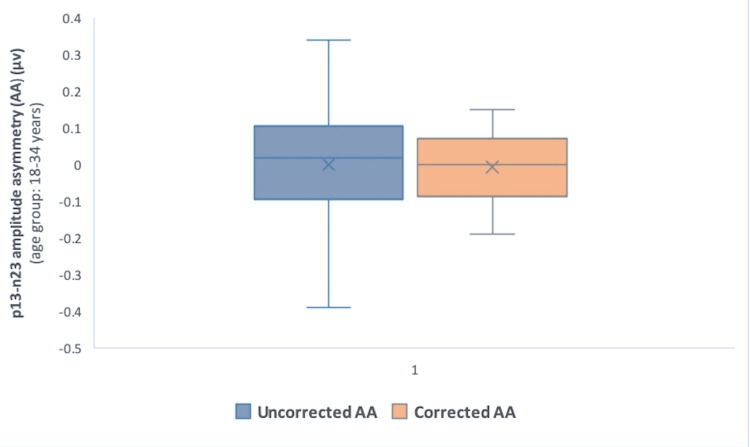
Background and objective Cervical vestibular-evoked myogenic potential (cVEMP) tests have attracted significant interest as clinical measures of vestibular function recently. A detailed knowledge of the potential individual factors influencing the cVEMP response is, however, essential for the reliability of the test. Hence, we aimed to analyze the trends of different cVEMP parameters with regard to changes in age and gender, under standard recording conditions. Methods cVEMP was conducted on 60 participants aged 18-60 years during the period from April 2023 to March 2024. cVEMP parameters, including response rates, amplitude, interaural amplitude asymmetry, threshold, threshold asymmetry, and latencies, were investigated for the impact of aging and gender differences. One-way ANOVA and Kruskal-Wallis tests were performed for the comparison between the age groups, while unpaired t-test and Kruskal-Wallis test were employed to find the gender differences in cVEMP parameters. Pearson correlation analysis was performed to assess the relationship between age and cVEMP parameters. Statistical significance was set at a p-value of 0.05. Results cVEMP response rate was 100 % in all the age groups. Significant differences were found in terms of p13-n23 amplitude and threshold (both right and left ear) between the age groups (p<0.001) (Kruskal-Wallis test). A significant negative correlation was found between age and both uncorrected and corrected amplitude in both the right ear (r = -0.73, p<0.001) and the left ear (r = -0.75, p<0.001). A significant positive correlation was observed between age and thresholds in both the right ear (r = 0.66, p<0.001) and the left ear (r = 0.75, p<0.001). There were no significant variations regarding p13 and n23 latencies, interaural amplitude asymmetry, and threshold asymmetry among the age groups (p>0.05) (one-way ANOVA) (Kruskal-Wallis test). Gender did not demonstrate variations in the cVEMP parameters tested (p>0.05) (unpaired t test and Kruskal-Wallis test). Conclusions cVEMP had an absolute detection rate in the age groups studied. However, a remarkable age-related decline in p13-n23 amplitude (corrected and uncorrected) and the threshold values highlights the importance of effective consideration of changes in age for optimizing the clinical evaluation. p13 and n23 latencies, and amplitude asymmetry were relatively stable with increasing age. The findings related to cVEMP evoked with 500 Hz short tone burst stimuli in adults (aged 18-60 years) can be utilized in the regional clinical settings.
Keywords: age; amplitude; amplitude asymmetry; cvemp; gender; latency; sternocleidomastoid; threshold; vestibular evoked myogenic potentials.
Copyright © 2025, Pandey et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institute’s Human Ethics Committee (IHEC), AIIMS Gorakhpur issued approval IHEC/AIIMS-GKP/BMR/123/2023. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures








Similar articles
-
Amplitude normalization reduces cervical vestibular evoked myogenic potential (cVEMP) amplitude asymmetries in normal subjects: proof of concept.J Am Acad Audiol. 2014 Mar;25(3):268-77. doi: 10.3766/jaaa.25.3.6. J Am Acad Audiol. 2014. PMID: 25032971
-
Cervical vestibular evoked myogenic potentials in 3-month-old infants: Comparative characteristics and feasibility for infant vestibular screening.Front Neurol. 2022 Sep 29;13:992392. doi: 10.3389/fneur.2022.992392. eCollection 2022. Front Neurol. 2022. PMID: 36247765 Free PMC article.
-
Cervical Vestibular Evoked Myogenic Potentials (cVEMPs) Evoked by Air-Conducted Stimuli in Patients with Functional Neck Dissection.J Natl Med Assoc. 2018 Jun;110(3):281-286. doi: 10.1016/j.jnma.2017.06.009. Epub 2017 Jul 12. J Natl Med Assoc. 2018. PMID: 29778132
-
The effects of amplitude normalization and EMG targets on cVEMP interaural amplitude asymmetry.Ear Hear. 2013 Jul-Aug;34(4):482-90. doi: 10.1097/AUD.0b013e31827ad792. Ear Hear. 2013. PMID: 23361360
-
Cervical Vestibular Evoked Myogenic Potentials in Benign Paroxysmal Positional Vertigo: A Systematic Review and Meta-Analysis.Front Neurol. 2019 Oct 1;10:1043. doi: 10.3389/fneur.2019.01043. eCollection 2019. Front Neurol. 2019. PMID: 31632337 Free PMC article.
References
-
- Vestibular-evoked myogenic potentials: past, present and future. Rosengren SM, Welgampola MS, Colebatch JG. Clin Neurophysiol. 2010;121:636–651. - PubMed
-
- A critical review of the neurophysiological evidence underlying clinical vestibular testing using sound, vibration and galvanic stimuli. Curthoys IS. Clin Neurophysiol. 2010;121:132–144. - PubMed
-
- Vestibular-evoked myogenic potential thresholds normalize on plugging superior canal dehiscence. Welgampola MS, Myrie OA, Minor LB, Carey JP. Neurology. 2008;70:464–472. - PubMed
-
- Ocular and cervical vestibular-evoked myogenic potentials produced by air-and bone-conducted stimuli: comparative properties and effects of age. Rosengren SM, Govender S, Colebatch JG. Clin Neurophysiol. 2011;122:2282–2289. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous