

Voiding symptom severity varies independently from non-adrenergic prostate smooth muscle contractions in patients undergoing surgery for benign prostatic hyperplasia
- PMID: 40519781
- PMCID: PMC12162512
- DOI: 10.3389/fphys.2025.1612954
Voiding symptom severity varies independently from non-adrenergic prostate smooth muscle contractions in patients undergoing surgery for benign prostatic hyperplasia
Abstract
Background: Resistance of voiding symptoms to α1-blockers in benign prostatic hyperplasia (BPH) has been provisionally explained by non-adrenergic prostate smooth muscle contraction. Here, we examined relationships between contractions and voiding symptoms in prostate tissues from laser-enucleation.
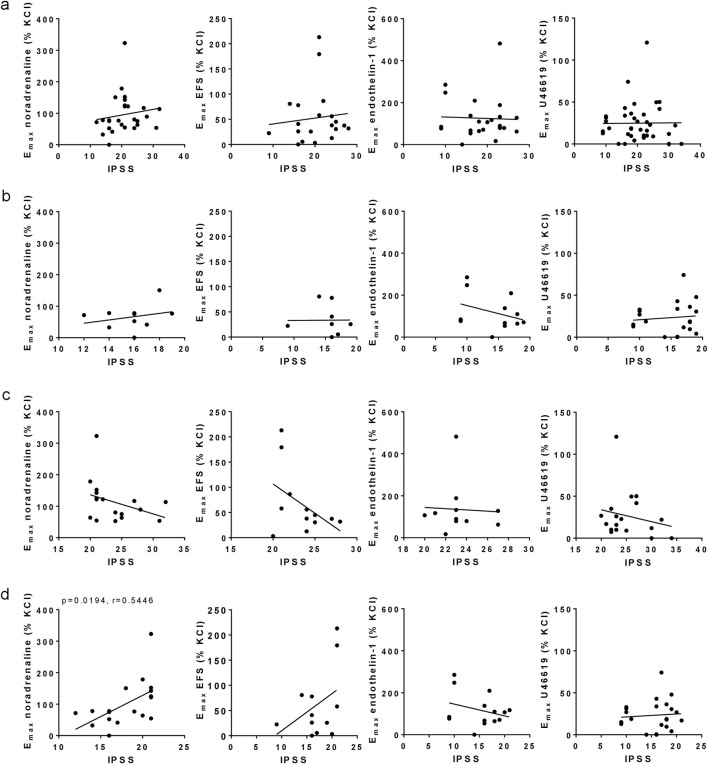
Methods: Tissues were obtained from holmium and thulium laser enucleation. Contractions were induced by endothelin-1, U46619, noradrenaline and electric field stimulation (EFS). Emax values were analyzed for correlation with international prostate symptom score (IPSS), and compared to tissues from patients without surgery for BPH.
Results: Noradrenaline- and EFS-induced contractions were higher with severe (IPSS 20-35) than moderate symptoms (IPSS 8-19) (Emax noradrenaline 66% vs 113% of KCl-induced contractions; EFS 33% vs 66%). Endothelin-1- and U46619-induced contractions were already maximum with moderate symptoms (endothelin-1 117% moderate, 135% severe; U46619 23%, 27%). Within 8-21 points, IPSS increased with Emax values for noradrenaline and EFS (r = 0.545, r = 0.448), but not with endothelin-1- or U46619-induced contractions. Endothelin-1-induced contractions were similar to noradrenaline-induced contractions (Emax endothelin-1 126% of KCl, noradrenaline 96%), and exceeded EFS- (52%) and U46619-induced contractions (25%). Emax values for endothelin-1 were similar between laser-enucleated patients and patients without surgery for BPH (127%), while Emax values for U46619 were higher in tissues from patients without surgery for BPH (59%) compared to laser-enucleated tissues.
Conclusion: Symptom severity increases with α1-adrenergic, but not with non-adrenergic contractions in patients undergoing surgery for BPH. Endothelin-1-induced contractions are similar to noradrenaline-induced contractions. Conditions necessitating BPH surgery may not necessarily depend on α1-adrenergic tone, but may involve non-adrenergic contractions or factors beyond contraction.
Keywords: benign prostatic hyperplasia (BPH); holmium laser enucleation of the prostate (HoLEP); human tissue; international prostate symptom score (IPSS); lower urinary tract symptoms (LUTS); smooth muscle contraction; voiding symptoms.
Copyright © 2025 Keller, Hu, Nicola, Berger, Tamalunas, Weinhold, Stief and Hennenberg.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures



Similar articles
-
Smooth muscle contractility of laser-enucleated prostate tissues and impacts of preoperative α1-blocker treatment in patients with and without catheterization.Sci Rep. 2025 Feb 10;15(1):4985. doi: 10.1038/s41598-025-88884-7. Sci Rep. 2025. PMID: 39929919 Free PMC article.
-
Non-Adrenergic, Tamsulosin-Insensitive Smooth Muscle Contraction is Sufficient to Replace α1 -Adrenergic Tension in the Human Prostate.Prostate. 2017 May;77(7):697-707. doi: 10.1002/pros.23293. Epub 2017 Jan 24. Prostate. 2017. PMID: 28116771
-
New strategies for inhibition of non-adrenergic prostate smooth muscle contraction by pharmacologic intervention.Prostate. 2019 May;79(7):746-756. doi: 10.1002/pros.23780. Epub 2019 Feb 27. Prostate. 2019. PMID: 30811062
-
Thulium Fiber Versus Holmium:Yttrium-aluminum-garnet Laser for Endoscopic Enucleation of the Prostate: A Systematic Review and Meta-analysis.Eur Urol Focus. 2024 Dec;10(6):914-921. doi: 10.1016/j.euf.2024.06.005. Epub 2024 Jun 18. Eur Urol Focus. 2024. PMID: 38897872
-
Phosphodiesterase inhibitors for lower urinary tract symptoms consistent with benign prostatic hyperplasia.BJU Int. 2019 Jul;124(1):27-34. doi: 10.1111/bju.14689. Epub 2019 Mar 11. BJU Int. 2019. PMID: 30681264
References
-
- Bailey K., Abrams P., Blair P. S., Chapple C., Glazener C., Horwood J., et al. (2015). Urodynamics for Prostate Surgery Trial; Randomised Evaluation of Assessment Methods (UPSTREAM) for diagnosis and management of bladder outlet obstruction in men: study protocol for a randomised controlled trial. Trials 16, 567. 10.1186/s13063-015-1087-1 - DOI - PMC - PubMed
-
- Chapple C. R., Montorsi F., Tammela T. L., Wirth M., Koldewijn E., Fernandez Fernandez E., et al. (2011). Silodosin therapy for lower urinary tract symptoms in men with suspected benign prostatic hyperplasia: results of an international, randomized, double-blind, placebo- and active-controlled clinical trial performed in Europe. Eur. Urol. 59 (3), 342–352. 10.1016/j.eururo.2010.10.046 - DOI - PubMed
-
- Cindolo L., Pirozzi L., Fanizza C., Romero M., Tubaro A., Autorino R., et al. (2015a). Drug adherence and clinical outcomes for patients under pharmacological therapy for lower urinary tract symptoms related to benign prostatic hyperplasia: population-based cohort study. Eur. Urol. 68 (3), 418–425. 10.1016/j.eururo.2014.11.006 - DOI - PubMed
LinkOut - more resources
Full Text Sources