

Endovascular treatment of a craniocervical junction dural arteriovenous fistula associated with lateral medullary syndrome: A case report
- PMID: 40519844
- PMCID: PMC12166782
- DOI: 10.1016/j.radcr.2025.05.021
Endovascular treatment of a craniocervical junction dural arteriovenous fistula associated with lateral medullary syndrome: A case report
Abstract
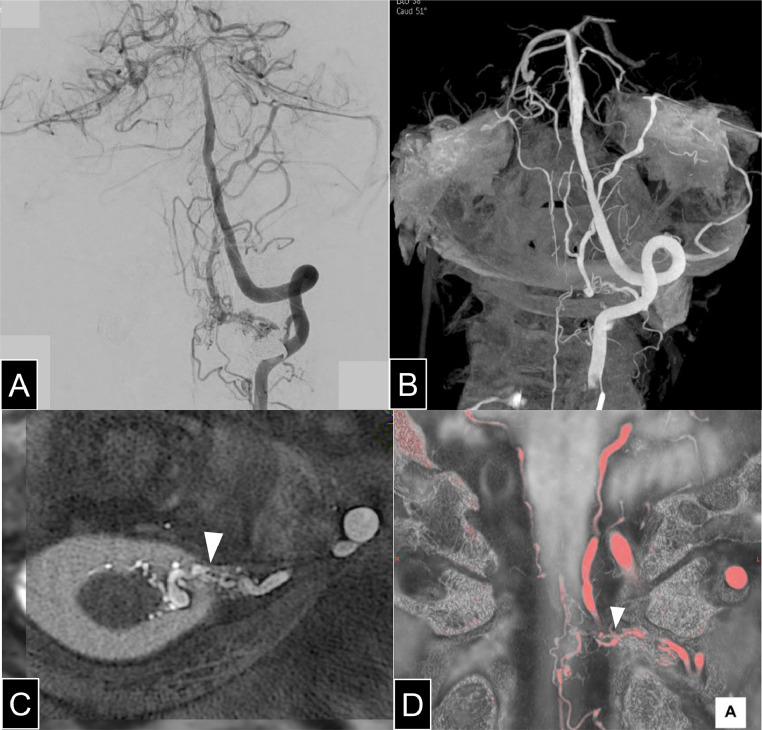
Intracranial dural arteriovenous fistulas (DAVFs) with drainage into the perimedullary veins have been reported to cause brainstem and spinal hemorrhages, subarachnoid hemorrhages, and progressive myelopathy. However, there have been no reports of craniocervical junction arteriovenous fistulas (CCJ-AVFs) complicated by lateral medullary syndrome (LMS) and subsequently treated. We present a case successfully treated with transvenous and transarterial embolization. A 67-year-old man presented with headache and dizziness was diagnosed with left LMS based on diffusion-weighted MRI. MRA ruled out vertebral artery dissection and posterior inferior cerebellar artery occlusion but suggested an arteriovenous shunt at the CCJ, which digital subtraction angiography confirmed as a DAVF fed by the radiculomeningeal artery with drainage into the anterior lateral spinal vein and deep brainstem veins. To minimize embolic complications, transvenous embolization with coils was performed first, followed by transarterial embolization with N-butyl cyanoacrylate. Postoperative MRI showed resolution of venous engorgement, and the patient was discharged without additional neurological deficits. This case highlights the potential role of AVF-induced venous engorgement in brainstem infarction and underscores the importance of early diagnosis and individualized treatment. A combined transvenous and transarterial approach can effectively control ascending venous outflow while minimizing procedural risks.
Keywords: Brainstem infarction; Craniocervical junction; Dural arteriovenous fistula; Endovascular treatment; Lateral medullary syndrome.
© 2025 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



Similar articles
-
Dural arteriovenous fistulas of the hypoglossal canal: systematic review on imaging anatomy, clinical findings, and endovascular management.J Neurosurg. 2015 Apr;122(4):883-903. doi: 10.3171/2014.10.JNS14377. Epub 2014 Nov 21. J Neurosurg. 2015. PMID: 25415064
-
The role of venous anatomy in guiding treatment approach for dural arteriovenous fistulas of the craniocervical junction; case series & systematic review.J Clin Neurosci. 2023 Apr;110:27-38. doi: 10.1016/j.jocn.2023.02.004. Epub 2023 Feb 12. J Clin Neurosci. 2023. PMID: 36787670
-
Transarterial Embolization of Intracranial Dural Arteriovenous Fistulas Cognard Type V With Direct Drainage Into the Perimedullary Veins: Case Report and Literature Review.Oper Neurosurg. 2024 Dec 1;27(6):765-771. doi: 10.1227/ons.0000000000001195. Epub 2024 Apr 30. Oper Neurosurg. 2024. PMID: 38687051 Review.
-
Spinal dural arteriovenous fistulas presenting as intracranial subarachnoid hemorrhage: A systematic review.Interv Neuroradiol. 2025 Jul 15:15910199251328721. doi: 10.1177/15910199251328721. Online ahead of print. Interv Neuroradiol. 2025. PMID: 40660916 Free PMC article. Review.
-
Angioarchitecture Classification and Treatment Modalities of Craniocervical Junction Arteriovenous Fistulas: A Cohort Study of 155 Patients.Neurosurgery. 2024 Sep 1;95(3):692-701. doi: 10.1227/neu.0000000000002939. Epub 2024 Apr 15. Neurosurgery. 2024. PMID: 39145652
References
-
- Hiramatsu M., Sugiu K., Ishiguro T., Kiyosue H., Sato K., Takai K., et al. Angioarchitecture of arteriovenous fistulas at the craniocervical junction: a multicenter cohort study of 54 patients. J Neurosurg. 2018;128(6):1839–1849. - PubMed
-
- Endo T., Shimizu H., Sato K., Niizuma K., Kondo R., Matsumoto Y., et al. Cervical perimedullary arteriovenous shunts: a study of 22 consecutive cases with a focus on angioarchitecture and surgical approaches. Neurosurgery. 2014;75(3):238–249. discussion 49. - PubMed
-
- Willinsky R., Lasjaunias P., Terbrugge K., Hurth M. Angiography in the investigation of spinal dural arteriovenous fistula. A protocol with application of the venous phase. Neuroradiology. 1990;32(2):114–116. - PubMed
-
- Takai K. Update on the diagnosis and treatment of arteriovenous fistulas at the Craniocervical junction: a systematic review of 92 cases. J Neuroendovasc Ther. 2019;13(3):125–135.
Publication types
LinkOut - more resources
Full Text Sources
