

Tendon and ligament injuries of the finger and thumb in athletes: a narrative review
- PMID: 40520026
- PMCID: PMC12164644
- DOI: 10.1136/bmjsem-2025-002475
Tendon and ligament injuries of the finger and thumb in athletes: a narrative review
Abstract
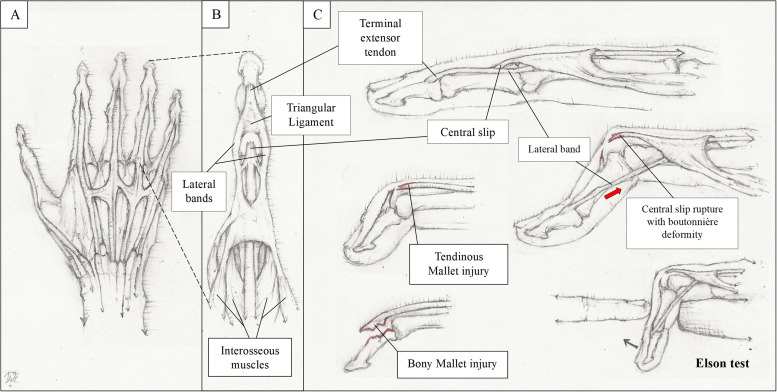
Acute finger and thumb injuries of the ligament and tendons are common. Indeed, a cross-sectional study in 2012 showed that they accounted for 38.4% of all upper extremity injury visits to the emergency room in the USA. Understanding the anatomy and mechanical functions of tendons and ligaments in the digits is crucial for recognising various types of injuries and their treatment. Treating an athlete with such conditions comes with the added pressure of ensuring a timely return to play. This review will cover the anatomy, diagnoses and management of select tendinous and ligamentous injuries of the fingers and thumb seen in athletes.
Keywords: Finger; Sporting injuries; Tendon.
Copyright © Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
None declared.
Figures



Similar articles
-
Sports Injury-Related Fingers and Thumb Deformity Due to Tendon or Ligament Rupture.Chin Med J (Engl). 2018 May 5;131(9):1051-1058. doi: 10.4103/0366-6999.230721. Chin Med J (Engl). 2018. PMID: 29692376 Free PMC article.
-
The athlete's hand: ligament and tendon injury.Semin Musculoskelet Radiol. 2012 Sep;16(4):338-49. doi: 10.1055/s-0032-1327007. Epub 2012 Oct 9. Semin Musculoskelet Radiol. 2012. PMID: 23047281 Review.
-
[Sports-related injuries of the thumb and fingers].Radiologie (Heidelb). 2023 Apr;63(4):284-292. doi: 10.1007/s00117-023-01127-6. Epub 2023 Mar 14. Radiologie (Heidelb). 2023. PMID: 36917239 Review. German.
-
Thumb Injuries in Athletes.Hand Clin. 2017 Feb;33(1):161-173. doi: 10.1016/j.hcl.2016.08.008. Hand Clin. 2017. PMID: 27886832 Review.
-
Finger Metacarpophalangeal Joint Injuries in Athletes: Evaluation, Diagnosis, Treatment, and Return to Play.J Am Acad Orthop Surg. 2023 Feb 15;31(4):e177-e188. doi: 10.5435/JAAOS-D-21-01031. J Am Acad Orthop Surg. 2023. PMID: 36757330 Review.
References
Publication types
LinkOut - more resources
Full Text Sources