

Preexisting statin therapy is not associated with reduced acute kidney injury following cardiac surgery: a retrospective analysis
- PMID: 40520192
- PMCID: PMC12162650
- DOI: 10.3389/fphar.2025.1613681
Preexisting statin therapy is not associated with reduced acute kidney injury following cardiac surgery: a retrospective analysis
Erratum in
-
Correction: Preexisting statin therapy is not associated with reduced acute kidney injury following cardiac surgery: a retrospective analysis.Front Pharmacol. 2025 Aug 19;16:1657887. doi: 10.3389/fphar.2025.1657887. eCollection 2025. Front Pharmacol. 2025. PMID: 40904556 Free PMC article.
Abstract
Background: Cardiac surgery-associated acute kidney injury (CSA-AKI) is one of the most prevalent forms of acute kidney injury (AKI) encountered in clinical practice, and its occurrence is significantly correlated with increased mortality and poor prognosis in patients. Although existing studies suggest that statins may influence the development of CSA-AKI through pleiotropic mechanisms, the findings from available studies and meta-analyses remain inconsistent. Therefore, the relationship between preexisting statin use and the risk of CSA-AKI development requires further investigation.
Methods: This study employed a retrospective cohort analysis based on the MIMIC-IV database. Patients undergoing ascending aortic surgery, coronary artery bypass grafting (CABG), or heart valve surgery were included and categorized based on preexisting statin use. Multifactorial logistic regression models were utilized to assess the association between statin use and outcome metrics, adjusting for confounding variables. To further validate the results, propensity score matching (PSM), sensitivity analyses, and subgroup analyses were conducted.
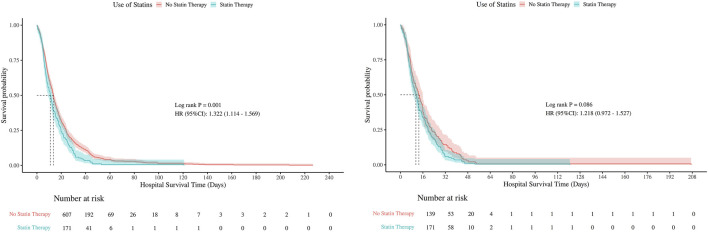
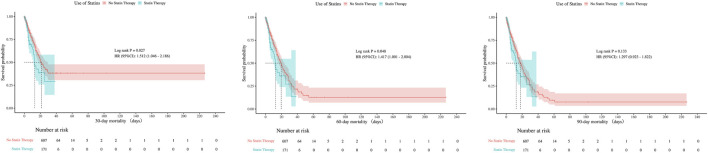
Results: A total of 4,783 patients were included, and the overall incidence of CSA-AKI was 30.02% (n = 1,436). Preliminary analysis showed that the incidence of AKI was significantly higher in the statin use group than in the non-use group (34.06% vs. 29.23%, P = 0.007). In the uncorrected model, statin use was associated with an elevated risk of AKI (OR = 1.25, 95% CI: 1.06-1.47); however, after multifactorial correction, the association was not statistically significant (OR = 1.00, 95% CI: 0.00-Inf, P = 1.000). Similarly, in the uncorrected model, statin use was associated with increased in-hospital mortality (OR = 1.28, 95% CI: 1.01-1.62) and ICU mortality (OR = 1.36, 95% CI: 1.07-1.72); however, after multifactorial correction, statin use was not significantly associated with in-hospital mortality (HR, 1.19; 95% CI, 0.92-1.53; P = 0.184) and ICU mortality (HR, 1.21; 95% CI, 0.94-1.55; P = 0.147) in the corrected model. PSM analysis (1:1 matching) further confirmed these findings (AKI: OR = 1.05, P = 0.621; in-hospital mortality: HR = 1.13, P = 0.438; ICU mortality: HR = 1.18, P = 0.299). None of the subgroup analyses (stratified by statin dose, AKI severity, and type of surgery) revealed significant interactions. Before PSM, no statistically significant differences were observed in 30-day (p = 0.126), 60-day (p = 0.372), or 90-day mortality (p = 0.652). After PSM, the mortality rates remained comparable between groups at all time points (30-day p = 0.297; 60-day p = 0.837; 90-day p = 0.966).
Conclusion: Preexisting statin use was not significantly associated with the risk of developing CSA-AKI, in-hospital mortality, or ICU mortality after appropriate correction for confounding variables. Similarly, no significant associations were observed for 30-day, 60-day, or 90-day mortality outcomes. Sensitivity analyses and subgroup analyses consistently supported this conclusion, suggesting that statin use may not significantly impact clinical outcomes in patients undergoing cardiac surgery.
Keywords: AKI; CSA-AKI; MIMIC-IV; cardiac surgery; statins.
Copyright © 2025 Wang, Huang, Chen, Huang and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Allou N., Augustin P., Dufour G., Tini L., Ibrahim H., Dilly M. P., et al. (2010). Preoperative statin treatment is associated with reduced postoperative mortality after isolated cardiac valve surgery in high-risk patients. J. Cardiothorac. Vasc. Anesth. 24 (6), 921–926. 10.1053/j.jvca.2010.03.017 - DOI - PubMed
-
- Bangalore S., Fayyad R., Hovingh G. K., Laskey R., Vogt L., DeMicco D. A., et al. (2014). Statin and the risk of renal-related serious adverse events: analysis from the IDEAL, TNT, CARDS, ASPEN, SPARCL, and other placebo-controlled trials. Am. J. Cardiol. 113 (12), 2018–2020. 10.1016/j.amjcard.2014.03.046 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous