

A soft robotic "Add-on" for colonoscopy: increasing safety and comfort through force monitoring
- PMID: 40520673
- PMCID: PMC12165838
- DOI: 10.1038/s44182-025-00028-1
A soft robotic "Add-on" for colonoscopy: increasing safety and comfort through force monitoring
Abstract
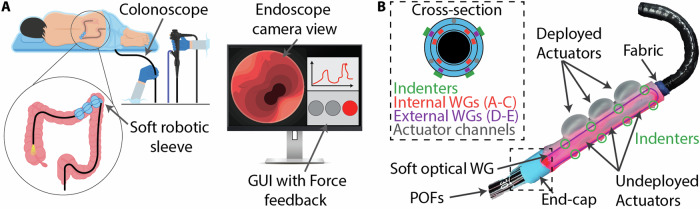
Colonoscopy is vital for diagnosing colorectal cancer, but limitations in instrument dexterity and sensor feedback can affect safety and patient comfort. We propose a disposable soft robotic "add-on" that attaches to existing endoscopic tools, enhancing safety without requiring custom instruments or workflow changes. The robot features soft optical sensors for 3D shape detection and force monitoring. If excessive force is detected, soft actuators redistribute pressure. A graphical interface provides real-time force data alongside the endoscope camera view. Validation experiments show accurate 3D shape reconstruction (8.51% curvature error, 9.67% orientation error) and force estimation up to 6 N with 3.38% accuracy. In-vitro tests confirm effective force redistribution, while ex-vivo tests on a bovine colon demonstrate smooth integration with minimal impact on the user learning curve. In-vivo swine studies validate safety and feasibility, confirming compatibility with existing tools and minimal disruption to clinical workflows, ensuring an efficient colonoscopy experience.
Keywords: Biomedical engineering; Materials for devices; Mechanical engineering; Soft materials.
© The Author(s) 2025.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures








References
-
- Siegel, R. L., Wagle, N. S., Cercek, A., Smith, R. A. & Jemal, A. Colorectal cancer statistics, 2023. CA: Cancer J. Clin.73, 233–254 (2023). - PubMed
-
- Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics. CA: Cancer J. Clin74, 12–49 (2024). - PubMed
-
- Santucci, C. et al. European cancer mortality predictions for the year 2024 with focus on colorectal cancer. Ann. Oncol.35, 308–316 (2024). - PubMed
-
- Siegel, R. L., Miller, K. D., Fuchs, H. E. & Jemal, A. Cancer statistics, 2023. CA: Cancer J. Clin.73, 17–48 (2023). - PubMed
LinkOut - more resources
Full Text Sources