

Analysis and comparison of the trends in burden of atrial fibrillation/atrial flutter in China and worldwide from 1990 to 2021 and predictions to 2036 of China
- PMID: 40520932
- PMCID: PMC12162966
- DOI: 10.3389/fcvm.2025.1540750
Analysis and comparison of the trends in burden of atrial fibrillation/atrial flutter in China and worldwide from 1990 to 2021 and predictions to 2036 of China
Abstract
Background: It is essential to analyze the burden, trends, and inequalities of atrial fibrillation/flutter (AF/AFL) in China and to predict future trends, with the aim of raising awareness about risk factors and exploring strategies to control the significant disease burden.
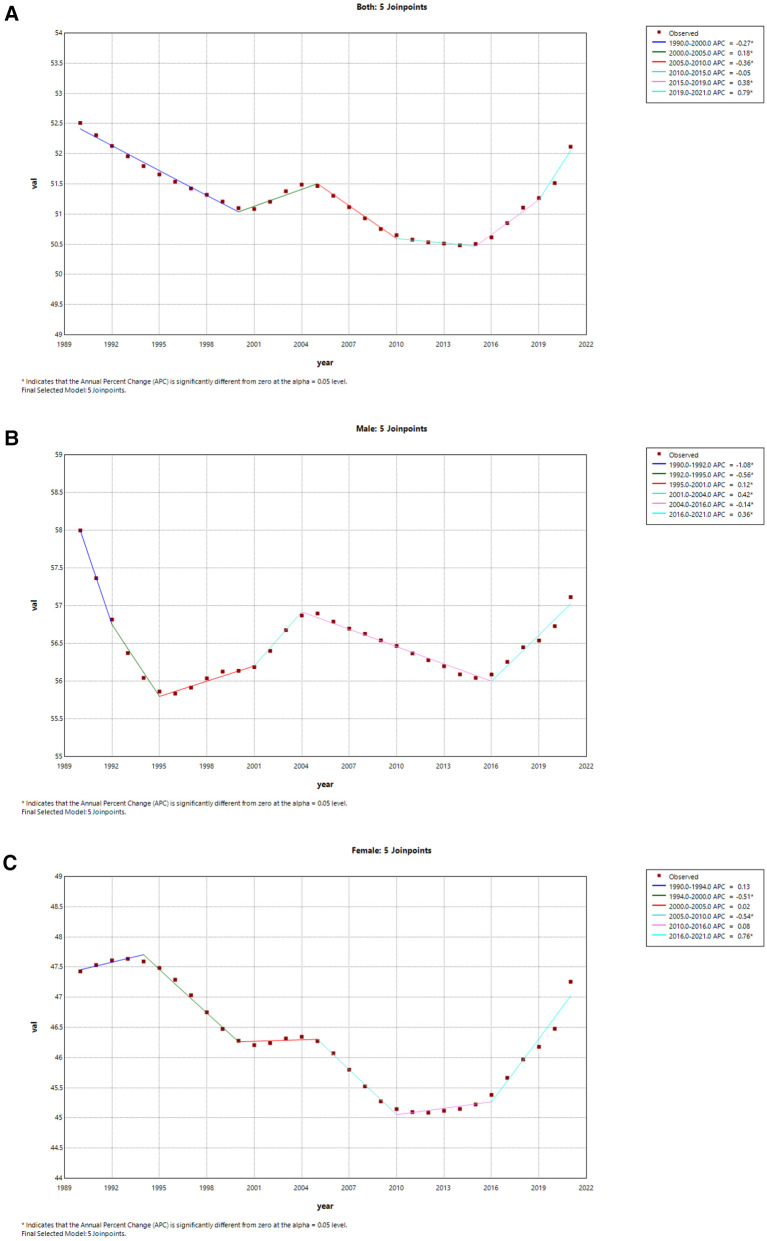
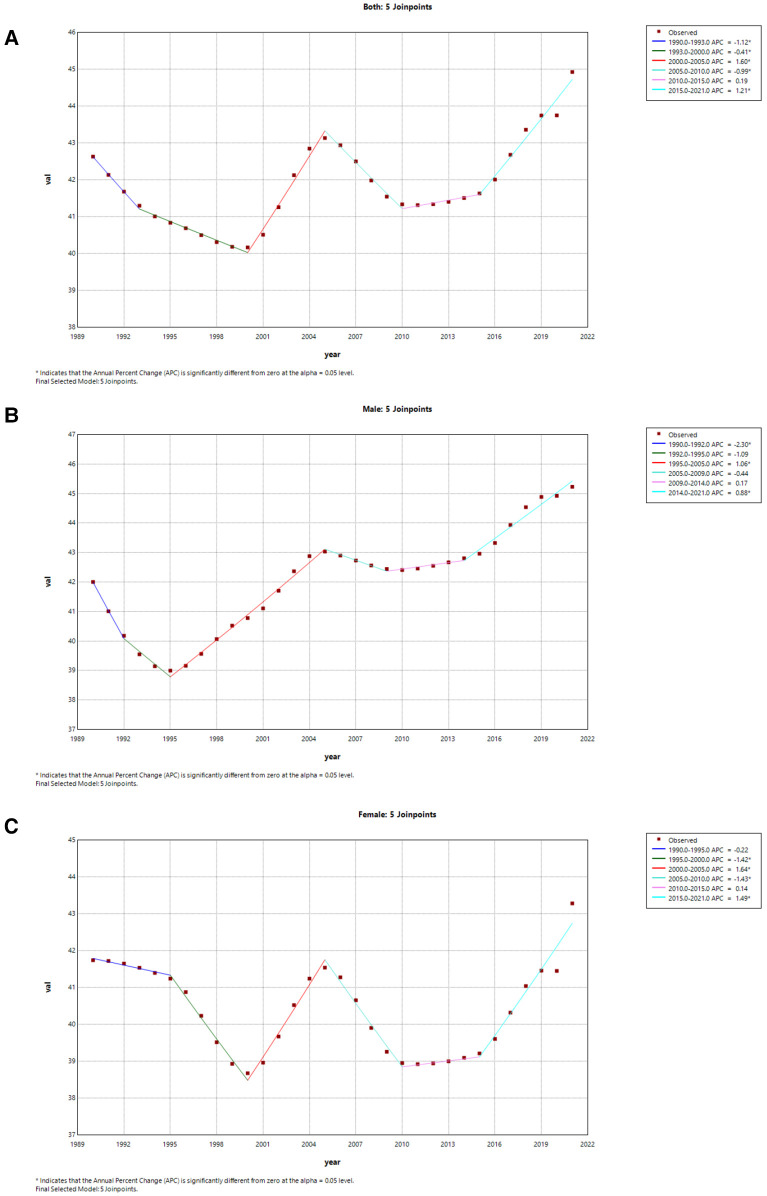
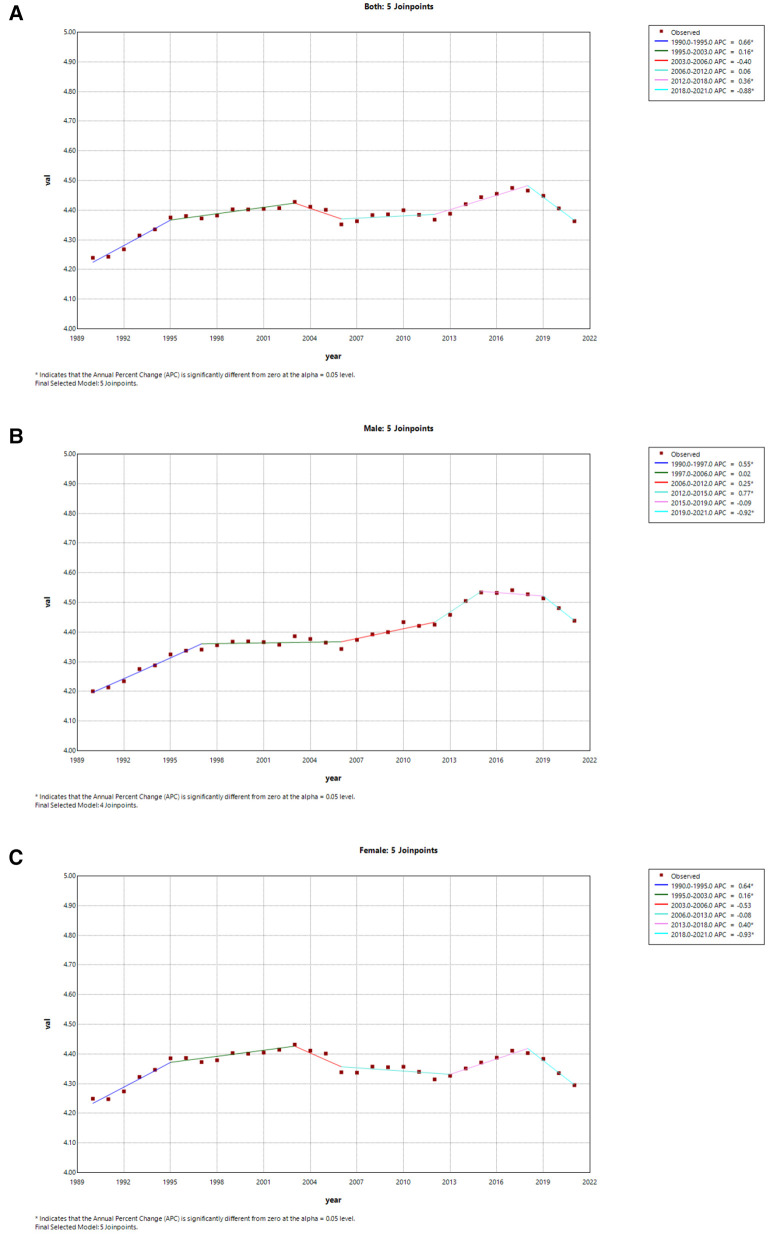
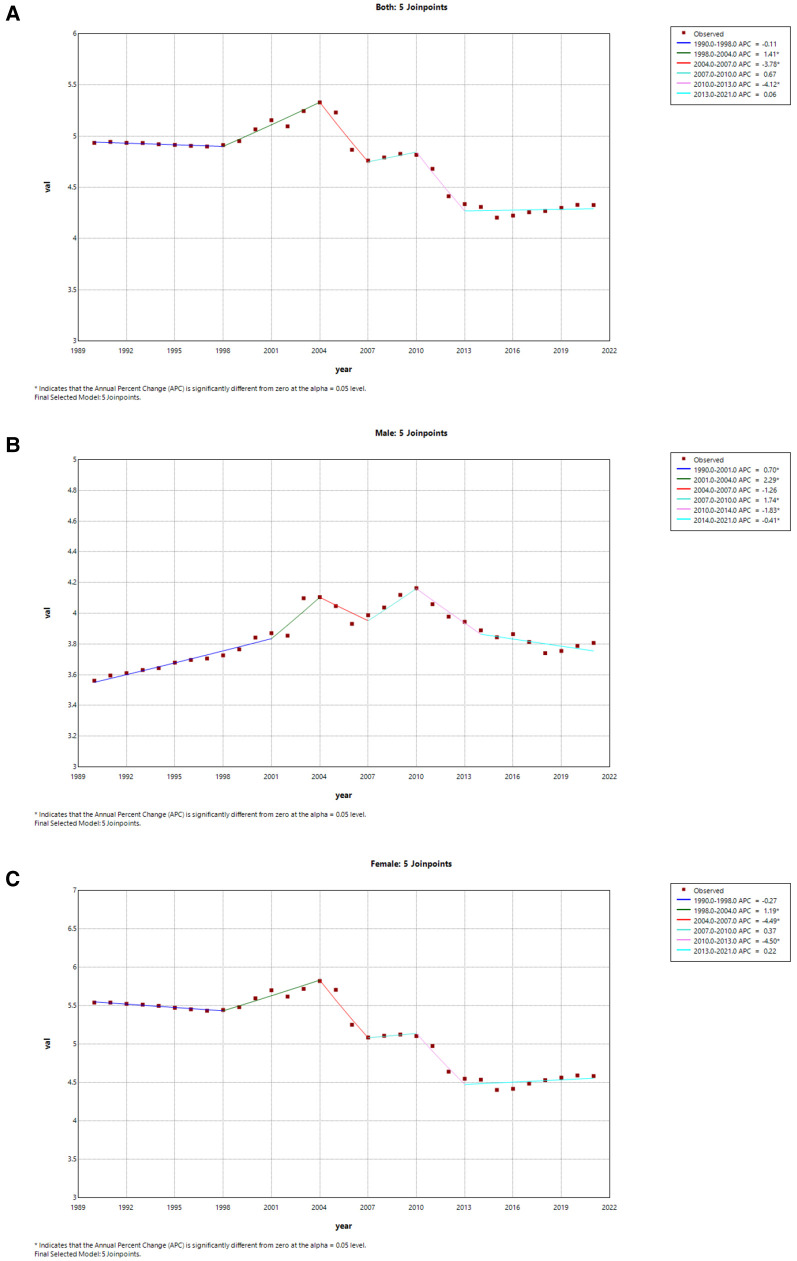
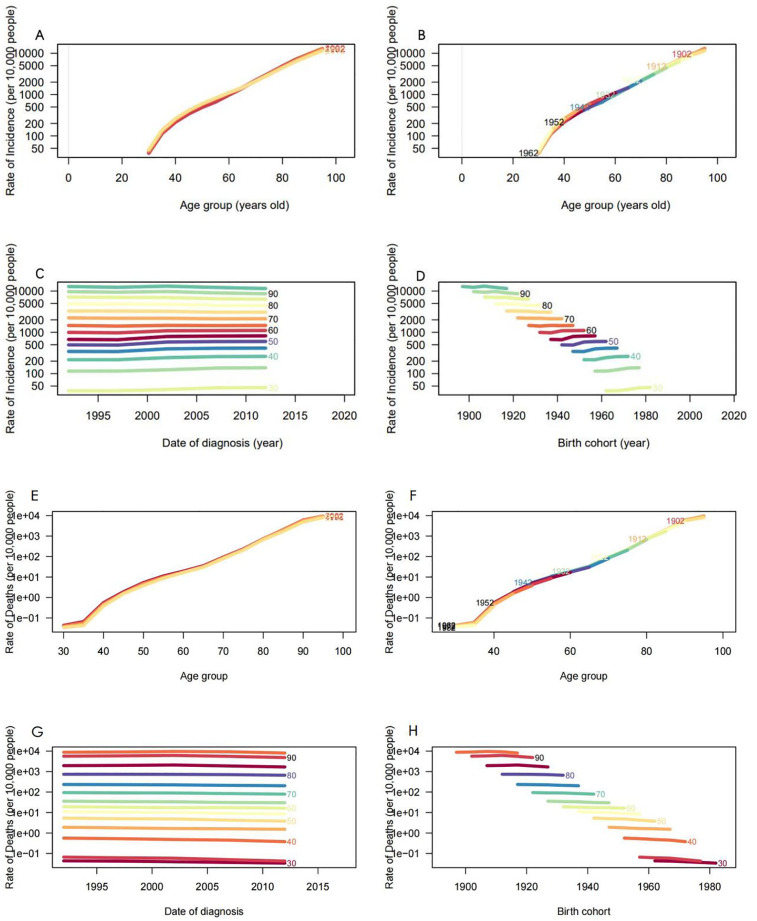
Methods: Data pertaining to AF/AFL were extracted from the comprehensive dataset of the Global Burden of Disease, Injuries, and Risk Factors Study 2021 (GBD 2021). Furthermore, we analyzed the epidemiological characteristics of AF/AFL and compared them to global prevalence trends, employing joinpoint regression, decomposition, age-period-cohort (apc), and cross-country inequality analysis methods. Concurrently, we utilized a Bayesian age-period-cohort (BAPC) analysis to forecast the age-standardized incidence rate (ASIR) of AF/AFL in China over the subsequent 15 years.
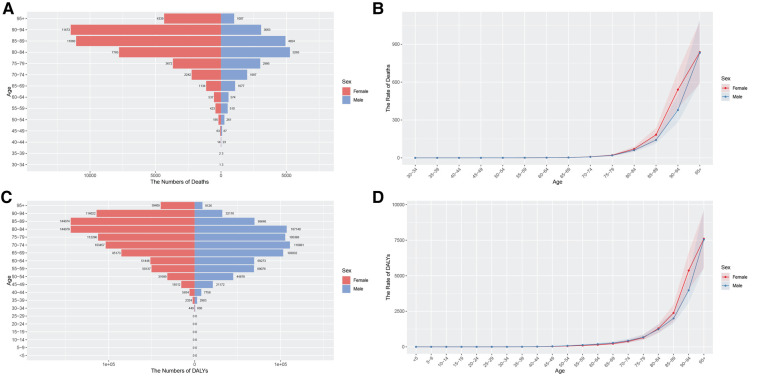
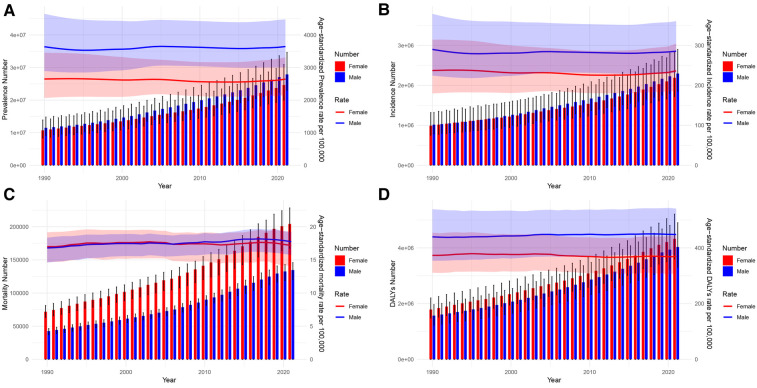
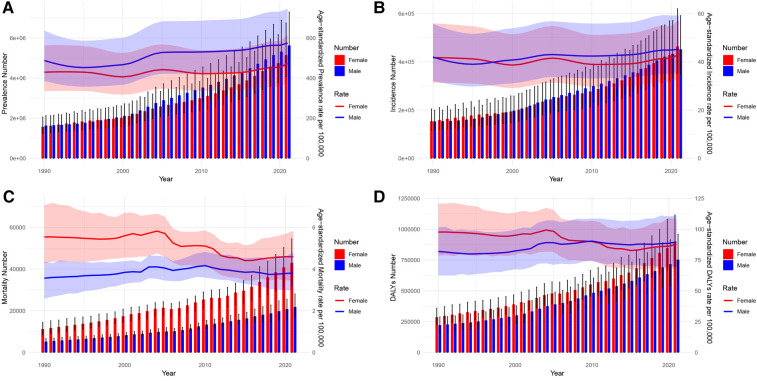
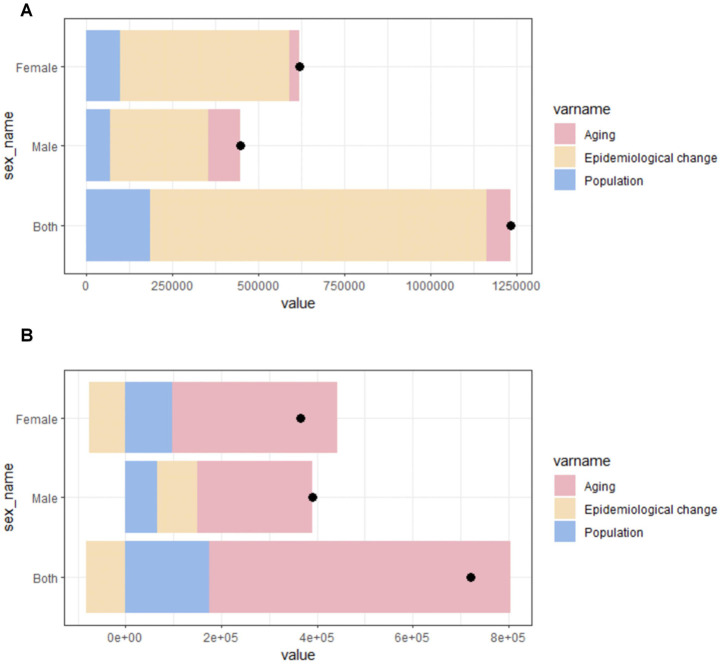
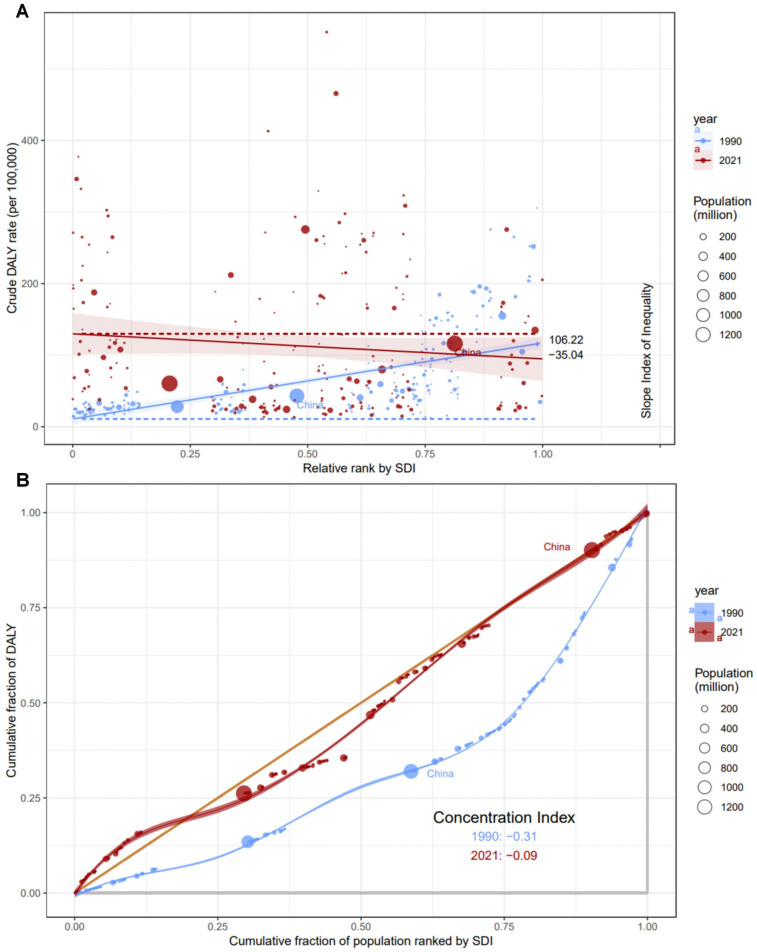
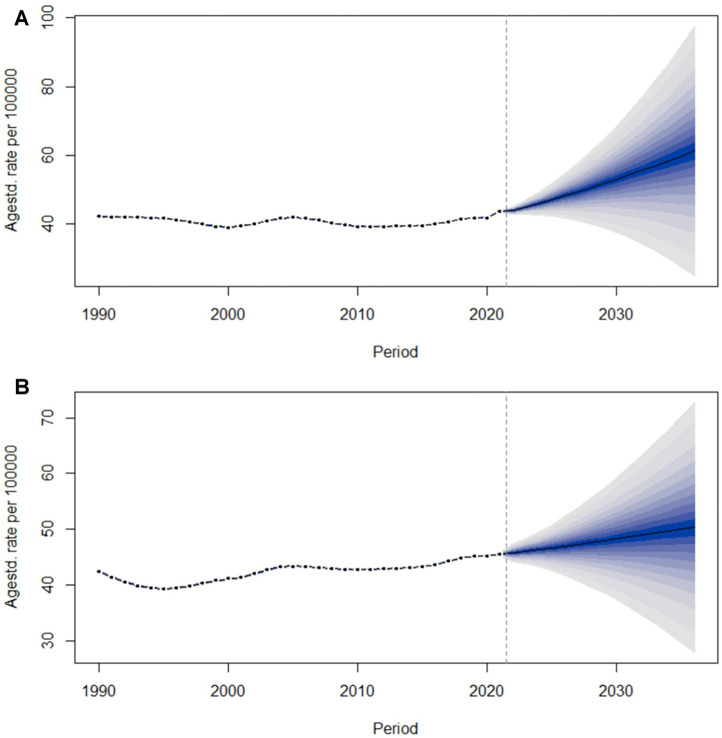
Results: Globally, in 2021, there were 52.55 million [95% uncertainty interval (UI): 43.14 to 64.96] prevalent cases, 4.48 million (95% UI: 3.61 to 5.71) incident cases, 0.34 million (95% UI: 0.28 to 0.37) deaths, and 8.36 million (95% UI: 6.97 to 10.13) DALYs. In China, during the same year, there were 10.78 million (95% UI: 8.53 to 14.01) prevalent cases, 0.92 million (95% UI: 0.71 to 1.20) incident cases, 0.06 million (95% UI: 0.05 to 0.08) deaths, and 1.65 million (95% UI: 1.30 to 2.06) DALYs. The average annual percentage change (AAPC) in age-standardized incidence and mortality rates for AF/AFL were -0.02 (95% CI: -0.05, 0) and 0.11 (95% CI: 0.03, 0.18) globally, and 0.16 (95% CI: 0.05, 0.26) and -0.45 (95% CI: -0.78, -0.12) in China, respectively. Decomposition analysis revealed epidemiological shifts drive incidence rise, aging affects mortality. The Slope Index of Inequality (SII) 2021 was -35.04, and the Concentration Index (CI) was -0.09. The BAPC results indicated that the ASIR for males and females is expected to rise over the next 15 years.
Conclusion: The burden of AF/AFL continues to increase annually. Countries with medium to low Socio-Demographic Index (SDI) have a heavy disease burden. In recent years, the burden in Chinese females has begun to exceed that of males. Without effective measures, the ASIR of AF/AFL is projected to exhibit a continued upward trajectory.
Keywords: age-period-cohort (APC) analysis; atrial fibrillation/atrial flutter (AF/AFL); disability-adjusted life years (DALYs); global burden of disease (GBD); inequality; joinpoint regression; prediction; socio-demography index (SDI).
© 2025 Wang, Shi, Shen, Zhang, Fang, Hu and Lv.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2019.Europace. 2023 Mar 30;25(3):793-803. doi: 10.1093/europace/euac237. Europace. 2023. PMID: 36603845 Free PMC article.
-
Differences in global, regional, and national time trends in disability-adjusted life years for atrial fibrillation and flutter, 1990-2019: an age-period-cohort analysis from the 2019 global burden of disease study.Front Cardiovasc Med. 2024 Aug 29;11:1401722. doi: 10.3389/fcvm.2024.1401722. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39267808 Free PMC article.
-
Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2021.Europace. 2024 Jul 2;26(7):euae195. doi: 10.1093/europace/euae195. Europace. 2024. PMID: 38984719 Free PMC article.
-
Global and China trends and forecasts of disease burden for female lung Cancer from 1990 to 2021: a study based on the global burden of disease 2021 database.J Cancer Res Clin Oncol. 2025 Feb 8;151(2):68. doi: 10.1007/s00432-025-06084-2. J Cancer Res Clin Oncol. 2025. PMID: 39921760 Free PMC article. Review.
-
Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019.JAMA Oncol. 2022 Mar 1;8(3):420-444. doi: 10.1001/jamaoncol.2021.6987. JAMA Oncol. 2022. PMID: 34967848 Free PMC article.
References
-
- GBD 2019 Diseases and Injuries Collaborators, Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. 10.1016/S0140-6736(20)30925-9 - DOI - PMC - PubMed
-
- Naghavi M, Ong KL, Aali A, Ababneh HS, Abate YH, Abbafati C, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2100–32. 10.1016/S0140-6736(24)00367-2 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources