

Case report: A novel technique of robotic low-tension hiatal hernia repair using mediastinoplication
- PMID: 40521120
- PMCID: PMC12164190
- DOI: 10.1016/j.mex.2025.103376
Case report: A novel technique of robotic low-tension hiatal hernia repair using mediastinoplication
Abstract
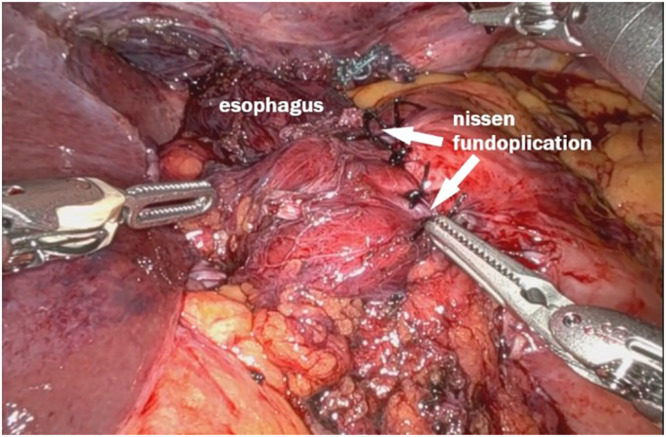
Surgery for giant hiatal hernias presents significant challenges, with laparoscopic surgery widely regarded as the gold standard. This approach typically involves complete resection of the hernia sac, thorough esophageal mobilization, tension-free closure of the diaphragmatic crura, and proper fundoplication. Despite various strategies to reduce recurrence, such as mesh reinforcement, there is no consensus on their superiority over traditional methods. Robotic surgery introduces greater precision, particularly in complex cases involving large hernias (grades III and IV). It facilitates safer dissections and more effective esophageal mobilization, challenging the concept of a short esophagus. A novel technique, mediastinoplication, addresses the positive abdominal-thoracic pressure gradient, a key factor in hernia recurrence. By reducing mediastinal dead space and approximating mediastinal structures, this technique aims to minimize tension on the crura and reduce recurrence, seroma, hematoma, and abscess. While further validation of mediastinoplication's long-term efficacy is needed, it adheres to fundamental surgical principles and offers a promising solution to high recurrence rates. Future studies are essential to establish its role in standard practice.•Introduces robotic mediastinoplication as a novel technique.•Robotic suturing increases the feasibility of suturing mediastinal structures that are inaccessible by traditional laparoscopic methods.•Mediastinoplication reduces tension, allowing a low-tension hiatal repair.
Keywords: Abdominal-thoracic pressure gradient; Diaphragmatic crura; Giant hiatal hernia; Innovative surgical technique; Low-tension repair; Mediastinal dissection; Mediastinoplication; Minimally invasive procedures; Recurrent hiatal hernia; Robotic Low-Tension Hiatal Hernia Repair Using Mediastinoplication; Robotic surgery.
© 2025 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures









Similar articles
-
Laparoscopic paraesophageal hernia repair: critical steps and adjunct techniques to minimize recurrence.Surg Laparosc Endosc Percutan Tech. 2013 Oct;23(5):429-35. doi: 10.1097/SLE.0b013e3182a12716. Surg Laparosc Endosc Percutan Tech. 2013. PMID: 24105280
-
Voluminous hiatal hernias - the role of robotic surgery.Innov Surg Sci. 2024 Jul 26;10(1):43-49. doi: 10.1515/iss-2023-0033. eCollection 2025 Mar. Innov Surg Sci. 2024. PMID: 40144781 Free PMC article. Review.
-
Hiatal Hernia Repair: A Century Between Soresi and da Vinci.Surg Clin North Am. 2025 Feb;105(1):125-142. doi: 10.1016/j.suc.2024.06.010. Epub 2024 Sep 6. Surg Clin North Am. 2025. PMID: 39523068 Review.
-
Laparoscopic hiatal hernia repair in patients with poor esophageal motility or paraesophageal herniation.Am Surg. 2001 Oct;67(10):987-91. Am Surg. 2001. PMID: 11603559
-
Operative trends and clinical outcomes of open, laparoscopic and robotic approaches to hiatal and paraoesophageal hernias- a study of 1834 patients.J Robot Surg. 2025 Apr 10;19(1):145. doi: 10.1007/s11701-025-02299-0. J Robot Surg. 2025. PMID: 40210798
References
-
- Leeder P., Smith G., Dehn T. Laparoscopic management of large paraesophageal hiatal hernia. Surg. Endosc. Other Intervent. Tech. 2003;17:1372–1375. - PubMed
-
- Akmaz B., Hameleers A., Boerma E.G., Vliegen R.F.A., Greve J.W.M., Meesters B., et al. Hiatal hernia recurrences after laparoscopic surgery: exploring the optimal technique. Surg. Endosc. 2023;37(6):4431–4442. - PubMed
-
- Hanna N.M., Kumar S.S., Collings A.T., Pandya Y.K., Kurtz J., Kooragayala K., et al. Management of symptomatic, asymptomatic, and recurrent hiatal hernia: a systematic review and meta-analysis. Surg. Endosc. 2024;38(6):2917–2938. - PubMed
-
- Ugliono E., Rebecchi F., Seno E., Morino M. Large hiatal hernia: minimizing early and long-term complications after minimally invasive repair. Mini-invasive Surgery. 2021:1–12.
-
- Chaudhry S., Farsi S., Nakanishi H., Parmar C., Ghanem O.M., Clapp B. Ligamentum teres augmentation for hiatus hernia repair after bariatric surgery: a systematic review and meta-analysis. Surg. Laparosc. Endosc. Percutaneous Tech. 2024;34(4):394–399. - PubMed
LinkOut - more resources
Full Text Sources
