

Non-invasive mapping of ventricular action potential waveforms reconstructed from clinical unshielded magnetocardiography. Potential diagnostic application and current limitations
- PMID: 40521306
- PMCID: PMC12167455
- DOI: 10.1016/j.ahjo.2025.100561
Non-invasive mapping of ventricular action potential waveforms reconstructed from clinical unshielded magnetocardiography. Potential diagnostic application and current limitations
Abstract
Objective: To evaluate the feasibility and limitations of reconstructing ventricular action potential waveforms using non-invasive, unshielded magnetocardiographic mapping (uMCG), highlighting differences between healthy individuals and patients, even at the current level of precision.
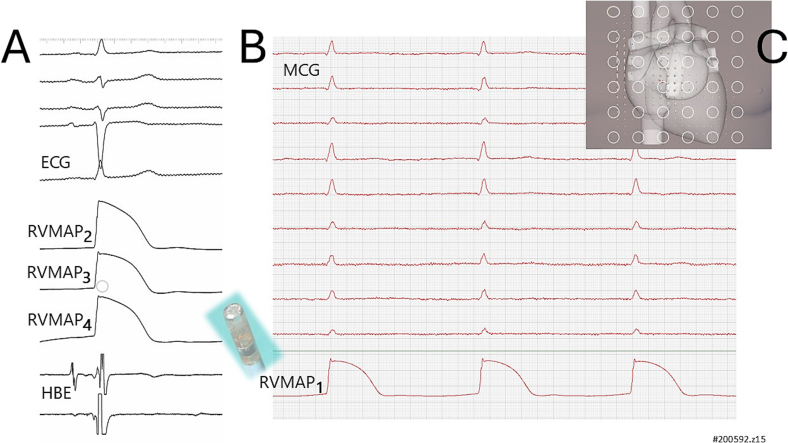
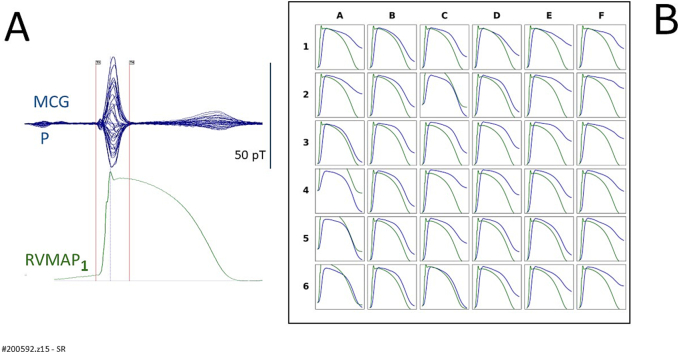
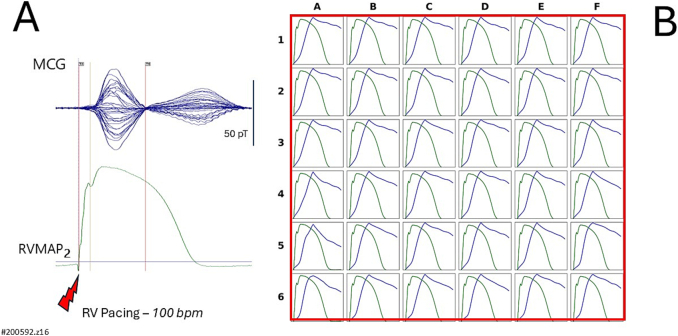
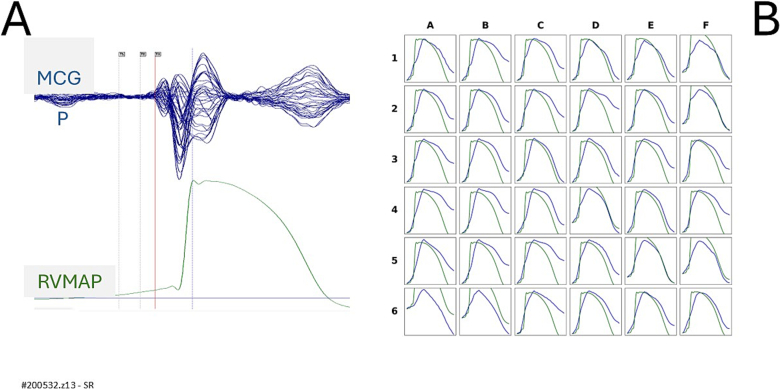
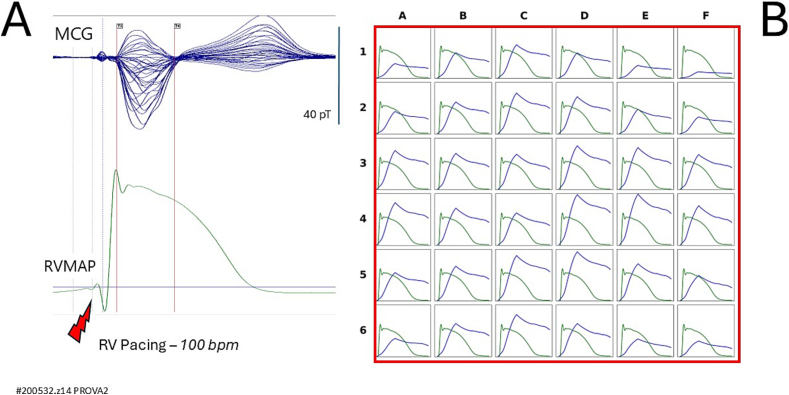
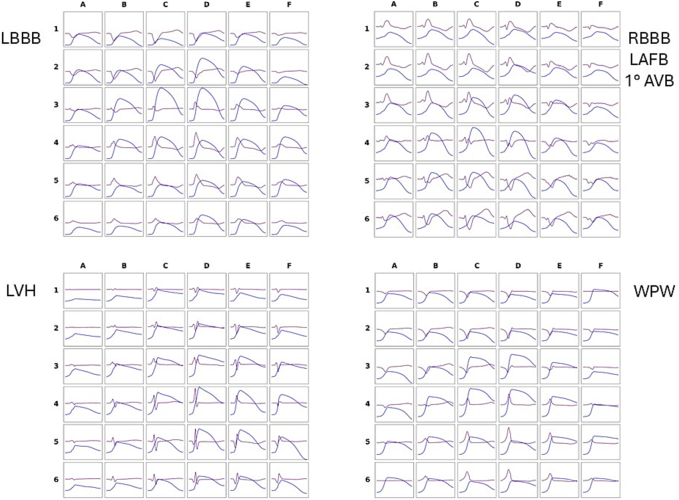
Methods: Clinical uMCG was performed using a 36-channel DC-SQUID system. The mathematical reconstruction method developed by Kandori et al. was applied to derive reconstructed ventricular action potential waveforms (rVAPw) from uMCG data in 10 healthy volunteers and 12 patients with various cardiac abnormalities. In four cases, simultaneous recordings of uMCG and right ventricular monophasic action potentials (RVMAP) were obtained using an amagnetic catheter technique.
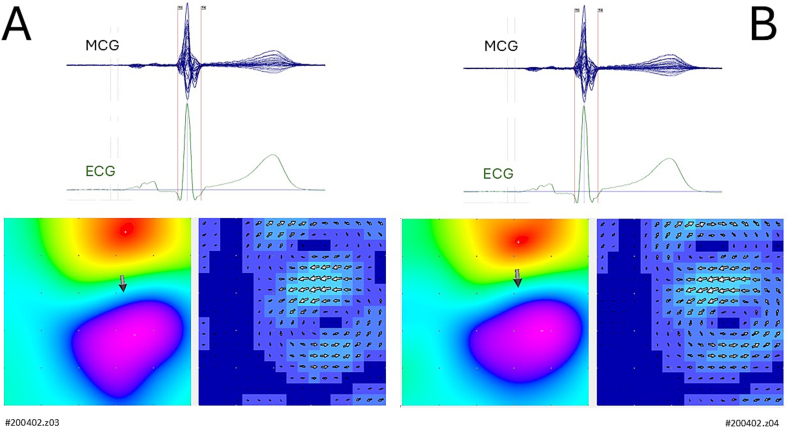
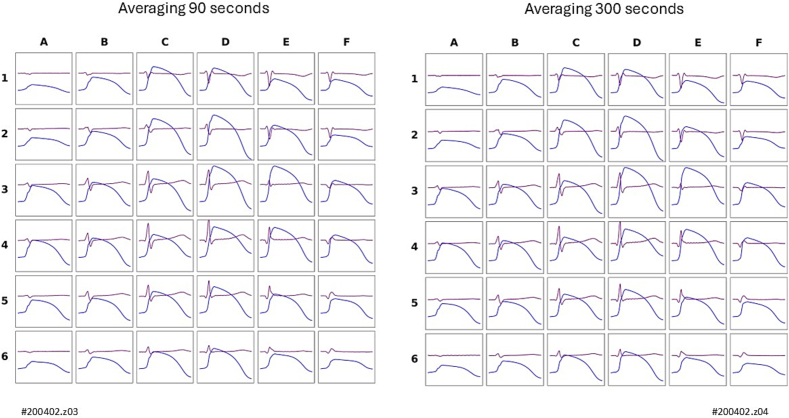
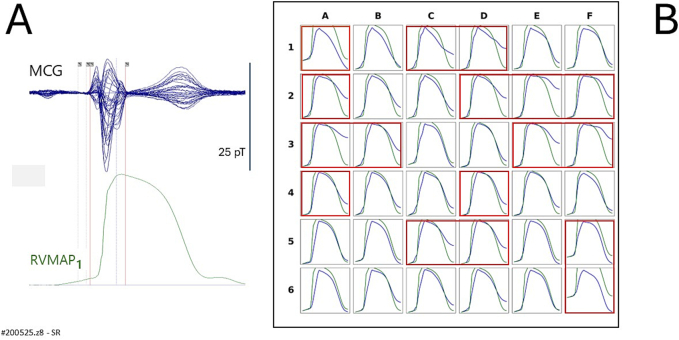
Results: Reconstruction of rVAPw from uMCG signals was feasible in all subjects. Waveforms derived from 90-s averaged uMCG signals were comparable to those obtained with 300-s averages. The rVAPw closely matched the simultaneously recorded RVMAP waveforms. Compared to healthy individuals, patients showed a significant prolongation of rVAPw phase-0 (p < 0.01) and a trend toward increased total duration (p = 0.06), demonstrating the method's sensitivity to electrophysiological abnormalities.
Conclusions: While incomplete rVAPw at some MCG mapping sites reflects the current spatial resolution limitations of the uMCG array, the close alignment between rVAPw and RVMAP recordings suggests that 90-s uMCG acquisitions may suffice for reliable, non-invasive imaging of ventricular action potentials in clinical practice. These findings support further development of MCG technology as a medical device uniquely suited to bridge experimental and clinical applications by enabling non-invasive rVAPw mapping in patients. Future improvements in sensor technology, mathematical modelling, and multimodal imaging may allow for near-cellular spatial resolution.
Keywords: Current arrow map; Magnetic reconstruction of ventricular action potential; Magnetocardiography; Magnetoionography; Monophasic action potential; Non-invasive multimodal imaging of electrophysiologic events.
© 2025 The Authors. Published by Elsevier Inc.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Percutaneous method for single-catheter multiple monophasic action potential recordings during magnetocardiographic mapping in spontaneously breathing rodents.Physiol Meas. 2012 Mar;33(3):521-34. doi: 10.1088/0967-3334/33/3/521. Epub 2012 Feb 29. Physiol Meas. 2012. PMID: 22373565
-
Magnetocardiography provides non-invasive three-dimensional electroanatomical imaging of cardiac electrophysiology.Anadolu Kardiyol Derg. 2007 Jul;7 Suppl 1:23-8. Anadolu Kardiyol Derg. 2007. PMID: 17584673
-
Magnetocardiographic pacemapping for nonfluoroscopic localization of intracardiac electrophysiology catheters.Pacing Clin Electrophysiol. 1998 Nov;21(11 Pt 2):2492-9. doi: 10.1111/j.1540-8159.1998.tb01207.x. Pacing Clin Electrophysiol. 1998. PMID: 9825373
-
Clinical magnetocardiography: the unshielded bet-past, present, and future.Front Cardiovasc Med. 2023 Aug 10;10:1232882. doi: 10.3389/fcvm.2023.1232882. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37636301 Free PMC article. Review.
-
[Development of three-dimensional analysis of current density distribution by 64-ch magentocardiography and clinical application].Rinsho Byori. 2008 Dec;56(12):1118-24. Rinsho Byori. 2008. PMID: 19175077 Review. Japanese.
References
-
- Lyon A.R., et al. 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the international cardio-oncology society (IC-OS): developed by the t. Eur. Heart J. 2022;43(41):4229–4361. doi: 10.1093/eurheartj/ehac244. - DOI - PubMed
-
- Fenici R., Bellocci F., Zecchi P. Monophasic action potential of human heart. Preliminary results with a new technique. Acta Med. Rom. 1973;11(5–6)
LinkOut - more resources
Full Text Sources
