

Evaluation of prosthetic dysfunction in the diagnosis of endocarditis associated to prosthetic pulmonary valve and pulmonary conduit
- PMID: 40521433
- PMCID: PMC12159197
- DOI: 10.1016/j.ijcchd.2025.100591
Evaluation of prosthetic dysfunction in the diagnosis of endocarditis associated to prosthetic pulmonary valve and pulmonary conduit
Abstract
Introduction: The number of cases of infective endocarditis associated to prosthetic pulmonary valves and pulmonary conduits (PPVIE) is likely to increase in the future. Transthoracic echocardiography (TTE) presents challenges in visualizing lesions suggestive of endocarditis in these patients. However, TTE may provide additional findings, such as prosthetic dysfunction, which can guide the diagnosis of this condition. The main objective of this study is to analyze prosthetic pulmonary valve dysfunction as an echocardiographic manifestation of PPVIE.
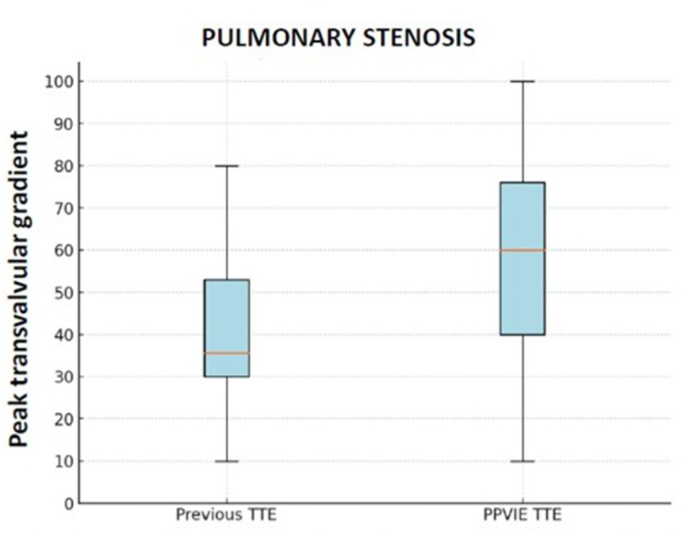
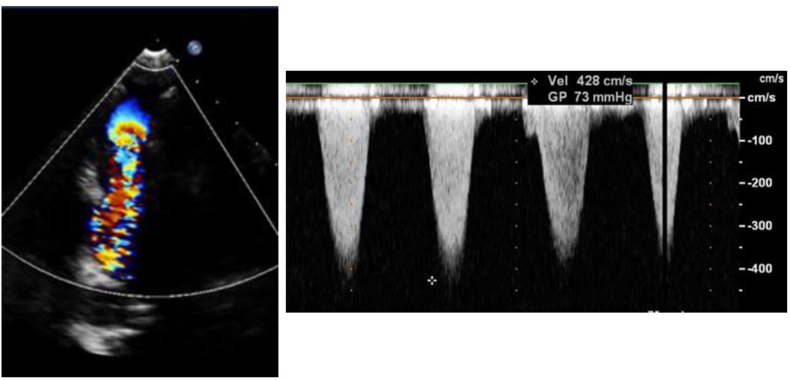
Methods: All cases of PPVIE (definite and possible, according to the modified Duke criteria) at Cruces University Hospital (Baracaldo, Spain) between January 2014 and July 2024 were included. Prosthetic dysfunction was defined as a peak transvalvular gradient (PTG) ≥25 mmHg for homografts and ≥40 mmHg for prosthetic pulmonary valves and bovine pulmonary conduits (stenosis) and/or pulmonary regurgitation (PR) moderate or severe. Number of cases of prosthetic dysfunction between the PPVIE episode and prior to the episode were compared. We analyzed the mechanisms of prosthetic dysfunction in the PPVIE episode.
Results: 14 cases of PPVIE were identified. In cases prior to the PPVIE episode, 42.9 % had prosthetic dysfunction, while in the PPVIE episode, 92.3 % had prosthetic dysfunction. Stenosis was a more frequent cause of valve dysfunction than PR.
Conclusions: Prosthetic dysfunction (due to stenosis or regurgitation) is a relevant finding in the diagnosis of PPVIE in cases where lesions suggestive of endocarditis are not visualised. Although not included in the Duke criteria, stenosis is a more frequent mechanism of dysfunction than PR.
Keywords: Infective endocarditis; Prosthetic dysfunction; Pulmonary valve prosthesis; Right ventricle to pulmonary artery conduit; Transcatheter pulmonary valve; Transtorathic echocardiography.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Van Melle J.P., Roos-Hesselink J.W., Bansal M., Kamp O., Meshaal M., Pudich J., Luksic V.R., Rodriguez-Alvarez R., Sadeghpour A., Hanzevacki J.S., Sow R., Timóteo A.T., Morgado M.T., De Bonis M., Laroche C., Boersma E., Lancellotti P., Habib G., Habib G. Infective endocarditis in adult patients with congenital heart disease. Int J Cardiol. 2022;370:178–185. doi: 10.1016/j.ijcard.2022.10.136. - DOI - PubMed
-
- Nordmeyer J., Ewert P., Gewillig M., AlJufan M., Carminati M., Kretschmar O., Uebing A., Dähnert I., Röhle R., Schneider H., Witsenburg M., Benson L., Gitter R., Bökenkamp R., Mahadevan V., Berger F. Acute and midterm outcomes of the post-approval MELODY Registry: a multicentre registry of transcatheter pulmonary valve implantation. Eur Heart J. 2019;40(27):2255–2264. doi: 10.1093/eurheartj/ehz201. - DOI - PubMed
-
- Miranda W.R., Connolly H.M., Bonnichsen C.R., DeSimone D.C., Dearani J.A., Maleszewski J.J., Greason K.L., Wilson W.R., Baddour L.M. Prosthetic pulmonary valve and pulmonary conduit endocarditis: clinical, microbiological and echocardiographic features in adults. Eur Heart J Cardiovasc Imaging. 2023;17(8):936–943. doi: 10.1093/ehjci/jew086. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
