

Device Selection Contributes to Operative Time Reduction in Laparoscopic Sacrocolpopexy
- PMID: 40521574
- PMCID: PMC12165672
- DOI: 10.4103/gmit.gmit_155_23
Device Selection Contributes to Operative Time Reduction in Laparoscopic Sacrocolpopexy
Abstract
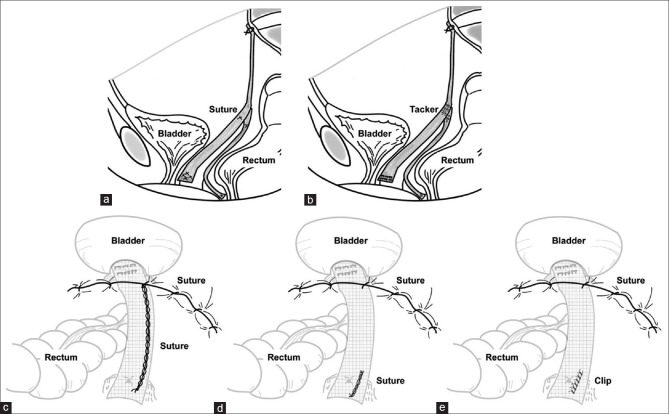
Objectives: The standard laparoscopic sacrocolpopexy (LSC) technique involves several suture fixation sites, which can prolong the operative time. This study aimed to investigate the extent to which the operative time could be shortened using devices such as tackers in sites where suture manipulation could be omitted.
Materials and methods: The study enrolled 82 patients who underwent LSC at our hospital between May 2016 and May 2022. The median operative time was 3.2 h (1.78-6.5 h). Changes in symptoms before and after surgery were measured using several questionnaires and 60-min pad weight testing among patient groups based on the device used.
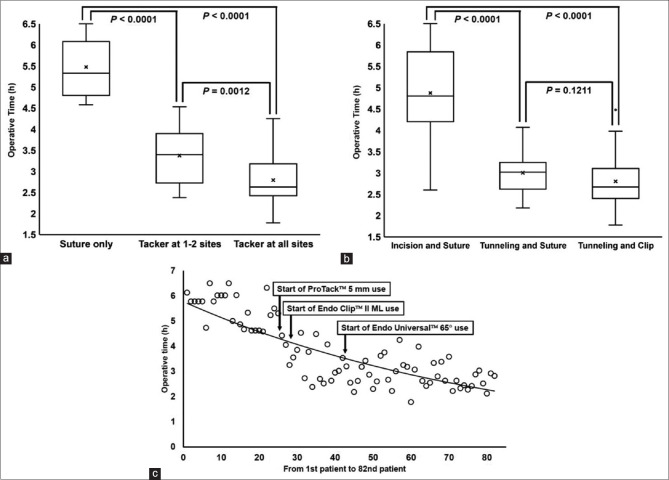
Results: Among the preoperative factors, no factors were found to be significantly correlated with the operative time (≥3.2 h or <3.2 h). As intraoperative factors, significant associations were found between the number of tackers used on the posterior vaginal wall, anterior vaginal wall, and cervix (0-3 locations), whether a device was used in mesh retroperitonealization, whether the first needle used to fix the anterior longitudinal ligament was successful, whether adhesion dissection was performed, and the type of sealing device. Among these factors, the use of tackers on the posterior wall, anterior wall, and cervix and the use of a device in mesh retroperitonealization were significantly associated with the operative time.
Conclusion: The use of easy-to-operate devices appeared to contribute to a shorter operative time in LSC.
Keywords: Fixation device; laparoscopic sacrocolpopexy; mesh retroperitonealization.
Copyright: © 2025 Gynecology and Minimally Invasive Therapy.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Vaginal-Assisted Laparoscopic Sacrocolpopexy (VALS) With Advanced Pelvic Organ Prolapse.J Minim Invasive Gynecol. 2025 Jan;32(1):12-13. doi: 10.1016/j.jmig.2024.07.015. Epub 2024 Jul 23. J Minim Invasive Gynecol. 2025. PMID: 39053845
-
Anatomical outcomes 1 year after pelvic organ prolapse surgery in patients with and without a uterus at a high risk of recurrence: a randomised controlled trial comparing laparoscopic sacrocolpopexy/cervicopexy and anterior vaginal mesh.Int Urogynecol J. 2019 Apr;30(4):545-555. doi: 10.1007/s00192-018-3702-7. Epub 2018 Jul 9. Int Urogynecol J. 2019. PMID: 29987345 Clinical Trial.
-
How to reduce the operative time of laparoscopic sacrocolpopexy?Gynecol Minim Invasive Ther. 2017 Jan-Mar;6(1):17-19. doi: 10.1016/j.gmit.2016.05.005. Epub 2016 Jul 5. Gynecol Minim Invasive Ther. 2017. PMID: 30254863 Free PMC article.
-
[Laparoscopic sacrocolpopexy for pelvic organ prolapse: guidelines for clinical practice].Prog Urol. 2016 Jul;26 Suppl 1:S27-37. doi: 10.1016/S1166-7087(16)30426-2. Prog Urol. 2016. PMID: 27595624 Review. French.
-
Laparoscopic sacrocolpopexy: A comprehensive literature review on current practice.Eur J Obstet Gynecol Reprod Biol. 2020 Feb;245:94-101. doi: 10.1016/j.ejogrb.2019.12.029. Epub 2019 Dec 26. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 31891897 Review.
Cited by
-
Advances in Women's Health Research.Gynecol Minim Invasive Ther. 2025 Jul 19;14(3):199-200. doi: 10.4103/gmit.GMIT-D-25-00044. eCollection 2025 Jul-Sep. Gynecol Minim Invasive Ther. 2025. PMID: 40786682 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Research Materials