

Circulating membrane aminophospholipids contribute to thrombotic risk in rheumatoid arthritis
- PMID: 40523622
- PMCID: PMC12273563
- DOI: 10.1016/j.jlr.2025.100842
Circulating membrane aminophospholipids contribute to thrombotic risk in rheumatoid arthritis
Abstract
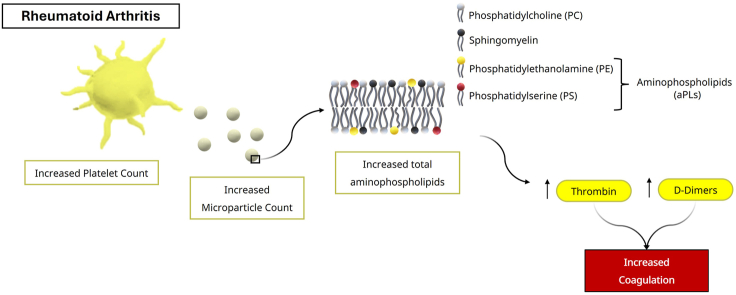
Patients with rheumatoid arthritis (RA) are at elevated risk of thrombotic events, yet the underlying mechanisms remain unknown. The contribution of the procoagulant membrane surface provided by aminophospholipids (aPLs) in driving thrombotic risk in RA has not been investigated. Specifically, neither the type of aPL exposed on circulating blood cell membranes in patients is characterized nor is their ability to support thrombin generation is known. Here, lipidomics was used to characterize the external-facing and total levels of aPL molecular species in RA, specifically phosphatidylserine and phosphatidylethanolamine on extracellular vesicles (EVs), platelets, and white blood cells (WBCs). The ability of the cells and EVs to support thrombin generation from patients and healthy controls was compared using an in vitro prothrombinase assay. RA patient plasma had significantly higher levels of thrombin-antithrombin and d-dimers, indicating increased thrombotic activity in vivo. Higher EV and platelet counts were seen in RA, but WBC counts were not elevated. EVs from RA patients supported higher levels of thrombin generation compared with healthy controls, whereas for platelets and WBC, thrombin generation was similar for both groups. EVs from RA patients also showed elevated external-facing phosphatidylserine molecular species, with total aPL also increased. For platelets and WBC, total and external-facing aPL levels were similar. Thrombin-antithrombin (TAT) complexes significantly correlated with EV particle counts, indicating that their circulating numbers are directly related to coagulation in vivo. Overall, our data suggest that elevated plasma EV levels in RA are a major source of procoagulant membranes, contributing to thrombotic risk in RA.
Keywords: aminophospholipids; extracellular vesicles; lipidomics; rheumatoid arthritis; thrombosis.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest E. C. has received research grants and honoraria from Abbvie, Alfasigma, Bio-Cancer, Biocon, Biogen, Chugai Pharma, Eli Lilly, Fresenius Kai, Galapagos, Gedeon Richter, Gilead, Inmedix, Janssen, Pfizer, Sanofi, UCB, and Viatris. S. A. J. has received funding support from Hoffman-La Roche, GlaxoSmithKline, Ferring Pharmaceuticals, Meastag Therapeutics, and NovImmune. S. A. J. has acted as an advisory consultant for Roche, Chugai Pharmaceuticals, NovImmune SA, Genentech, Sanofi Regeneron, Johnson & Johnson, Janssen Pharmaceuticals, Eleven Biotherapeutics, and Mab Design. V. O. D. is a consultant for Metasight.
Figures



Similar articles
-
Thrombin Generation Is Associated With Extracellular Vesicle and Leukocyte Lipid Membranes in Atherosclerotic Cardiovascular Disease.Arterioscler Thromb Vasc Biol. 2024 Sep;44(9):2038-2052. doi: 10.1161/ATVBAHA.124.320902. Epub 2024 Aug 1. Arterioscler Thromb Vasc Biol. 2024. PMID: 39087349 Free PMC article.
-
Extracellular histones: a unifying mechanism driving platelet-dependent extracellular vesicle release and thrombus formation in COVID-19.J Thromb Haemost. 2024 Sep;22(9):2514-2530. doi: 10.1016/j.jtha.2024.05.019. Epub 2024 May 28. J Thromb Haemost. 2024. PMID: 38815756 Free PMC article.
-
Thrombin generation and cell-dependent hypercoagulability in sickle cell disease.J Thromb Haemost. 2016 Oct;14(10):1941-1952. doi: 10.1111/jth.13416. Epub 2016 Aug 31. J Thromb Haemost. 2016. PMID: 27430959
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.Health Technol Assess. 2006 Nov;10(42):iii-iv, xi-xiii, 1-229. doi: 10.3310/hta10420. Health Technol Assess. 2006. PMID: 17049139
-
Antiplatelet and anticoagulant agents for primary prevention of thrombosis in individuals with antiphospholipid antibodies.Cochrane Database Syst Rev. 2018 Jul 13;7(7):CD012534. doi: 10.1002/14651858.CD012534.pub2. Cochrane Database Syst Rev. 2018. PMID: 30004572 Free PMC article.
Cited by
-
The risk of going outside: Amino phospholipids in rheumatoid arthritis.J Lipid Res. 2025 Jul 29;66(9):100870. doi: 10.1016/j.jlr.2025.100870. Online ahead of print. J Lipid Res. 2025. PMID: 40744314 Free PMC article. No abstract available.
References
-
- del Rincón I.D., Williams K., Stern M.P., Freeman G.L., Escalante A. High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheum. 2001;44:2737–2745. - PubMed
-
- Solomon D.H., Karlson E.W., Rimm E.B., Cannuscio C.C., Mandl L.A., Manson J.E., et al. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis. Circulation. 2003;107:1303–1307. - PubMed
-
- Carmassi F., De Negri F., Morale M., Puccetti R., Song K., Chung S. Assessment of coagulation and fibrinolysis in synovial fluid of rheumatoid arthritis patients. Fibrinolysis. 1994;8:162–171.
-
- Conn D.L., McDuffie F.C., Kazmier F.J., Schroeter A.L., Sun N.C.J. Coagulation abnormalities in rheumatoid disease. Arthritis Rheum. 1976;19:1237–1243. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
