

doi: 10.2340/actadv.v105.43419.
Four Cases of Prurigo Nodularis Requiring Nemolizumab due to Persistent Pruritus or Lesions after Dupilumab Treatment
Affiliations
- PMID: 40524402
- PMCID: PMC12186433
- DOI: 10.2340/actadv.v105.43419
Item in Clipboard
Four Cases of Prurigo Nodularis Requiring Nemolizumab due to Persistent Pruritus or Lesions after Dupilumab Treatment
Acta Derm Venereol.
.
No abstract available
Conflict of interest statement
YM and KI have received lecture fees from Maruho Co., which markets nemolizumab.
Figures

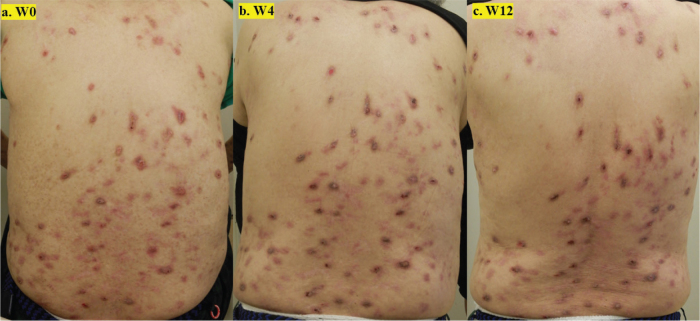
Clinical features of Patient 1 with prurigo nodularis who switched to nemolizumab after 12 weeks of dupilumab treatment due to persistent pruritus. (A) Baseline back lesions at the start of nemolizumab treatment. Before nemolizumab, dupilumab had led to partial flattening of the nodules, but numerous palpable lesions remained (PN-IGA 4), and pruritus remained severe (PP-NRS 7). (B) At Week 4, previously palpable nodules showed further flattening and signs of improvement (PN-IGA 3), though pruritus persisted (PP-NRS 5). (C) At Week 12, most nodules had flattened and evolved into post-inflammatory hyperpigmentation (PN-IGA 2), while pruritus remained stable (PP-NRS 6).
Clinical features of Patient 3 with prurigo nodularis who switched to nemolizumab after 13 weeks of dupilumab treatment due to persistent pruritus or skin lesions. (A) Baseline back lesions at the start of nemolizumab treatment. Before nemolizumab, despite prior dupilumab treatment, the nodules remained largely unchanged, with numerous palpable lesions (PN-IGA 4), and pruritus was extremely severe (PP-NRS 10). (B) At Week 4, the nodules showed no significant flattening and remained stable (PN-IGA 4), but pruritus improved markedly (PP-NRS 5). (C) At Week 12, some nodules showed signs of shrinkage, but many remained palpable (PN-IGA 4). However, pruritus continued to improve (PP-NRS 3).
Similar articles
-
Trial of Nemolizumab in Moderate-to-Severe Prurigo Nodularis.N Engl J Med. 2020 Feb 20;382(8):706-716. doi: 10.1056/NEJMoa1908316. N Engl J Med. 2020. PMID: 32074418 Clinical Trial.
-
Efficacy and safety of nemolizumab and topical corticosteroids for prurigo nodularis: results from a randomized double-blind placebo-controlled phase II/III clinical study in patients aged ≥ 13 years.Br J Dermatol. 2024 Jul 16;191(2):200-208. doi: 10.1093/bjd/ljae131. Br J Dermatol. 2024. PMID: 38629497 Clinical Trial.
-
A critical evaluation of nemolizumab for prurigo nodularis.Expert Rev Clin Immunol. 2024 Jun;20(6):577-587. doi: 10.1080/1744666X.2024.2306225. Epub 2024 Jan 19. Expert Rev Clin Immunol. 2024. PMID: 38217530 Review.
-
Phase 3 Trial of Nemolizumab in Patients with Prurigo Nodularis.N Engl J Med. 2023 Oct 26;389(17):1579-1589. doi: 10.1056/NEJMoa2301333. N Engl J Med. 2023. PMID: 37888917 Clinical Trial.
-
Nemolizumab: An Innovative Biologic Treatment to Control Interleukin 31, a Key Mediator in Atopic Dermatitis and Prurigo Nodularis.Actas Dermosifiliogr. 2022 Jul-Aug;113(7):674-684. doi: 10.1016/j.ad.2021.12.014. Epub 2021 Dec 23. Actas Dermosifiliogr. 2022. PMID: 35842249 Review. English, Spanish.
References
-
- Pereira MP, Steinke, S, Zeidler C, Forner C, Riepe C, Augustin M, et al. European Academy of Dermatology and Venereology European prurigo project: expert consensus on the definition, classification and terminology of chronic prurigo. J Eur Acad Dermatol Venereol 2018; 32: 1059-1065. 10.1111/jdv.14570 - DOI - PubMed
-
- Leis M, Fleming P, Lynde CW. Prurigo nodularis: review and emerging treatments. Skin Therapy Lett 2021; 26: 5–8. - PubMed
LinkOut - more resources
Full Text Sources
