

COTE and Pulmonary Comorbidities Predict Moderate-to-Severe Acute Exacerbation and Hospitalization in COPD
- PMID: 40524721
- PMCID: PMC12169424
- DOI: 10.2147/COPD.S518218
COTE and Pulmonary Comorbidities Predict Moderate-to-Severe Acute Exacerbation and Hospitalization in COPD
Abstract
Purpose: The aim of this study was to explore the predictive value of the chronic obstructive pulmonary disease (COPD) specific comorbidity test index (COTE) and pulmonary comorbidities for moderate-to-severe acute exacerbation and hospitalization in COPD patients.
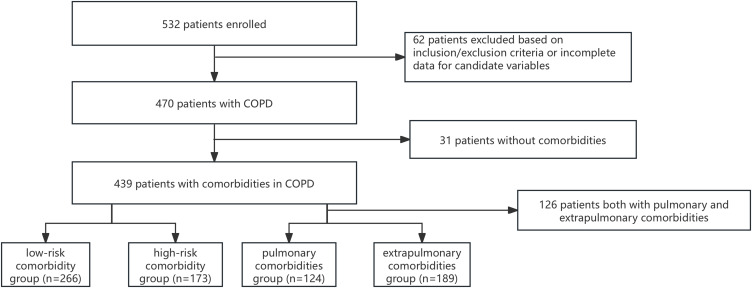
Patients and methods: This was a retrospective cohort study. We included 470 patients with stable COPD. Patients were divided into high or low-risk comorbidity group according to whether COTE score ≥4, and pulmonary comorbidities and extrapulmonary comorbidities group according to comorbidity origin. Moderate-to-severe acute exacerbation events and other clinical parameters were compared between groups. Multifactorial analysis and Lasso regression were used to screen risk factors and establish predictive models for moderate-to-severe acute exacerbation and hospitalization. The receiver operating characteristic (ROC) curve was used to assess the value COTE score and pulmonary comorbidities in predicting moderate-to-severe acute exacerbation and hospitalization.
Results: When compared with the low-risk comorbidity and extrapulmonary comorbidities group, the rate of patients with ≥2 moderate-to-severe acute exacerbations and requiring hospitalization due to acute exacerbations is higher in high-risk comorbidity and pulmonary comorbidities group (χ²=18.45, χ²=40.15, χ²=8.82, χ²=23.68). Multifactorial analysis showed that comorbid with asthma, lung cancer were risk factors for moderate-to-severe acute exacerbations, while asthma, bronchiectasis, lung cancer, and high COTE score were risk factors for patients requiring hospitalization due to acute exacerbations. The AUC for COTE > 5.5 and a combination of at least one pulmonary comorbidity as potential indication of moderate-to-severe acute exacerbations of COPD and hospitalization due to acute exacerbations was 0.667 (95% CI: 0.615, 0.719) and 0.740 (95% CI: 0.688, 0.792), respectively. The prediction models including COTE and pulmonary comorbidities can predict moderate-to-severe acute exacerbations (internal validation of AUC: 0.984, 95CI%: 0.964-1) and hospitalization (internal validation of AUC: 0.978, 95CI%: 0.959-0.998) of COPD.
Conclusion: COTE score and a combination of at least one pulmonary disease can predict the risk of moderate-to-severe acute exacerbations and hospitalization due to acute exacerbations in patients with COPD.
Keywords: acute exacerbation; chronic obstructive; comorbidity; hospitalization; pulmonary disease.
© 2025 Chen et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures








Similar articles
-
Association of Patient-Reported Outcome Patterns and Major Clinical Factors with Frailty in Stable COPD.Int J Chron Obstruct Pulmon Dis. 2025 Jun 12;20:1927-1937. doi: 10.2147/COPD.S517270. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40529222 Free PMC article.
-
FFMI: A Pivotal Indicator Bridging Pulmonary, Sleep, and Systemic Factors in COPD-OSA Overlap Patients.Int J Chron Obstruct Pulmon Dis. 2025 Jun 10;20:1843-1849. doi: 10.2147/COPD.S514400. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40524722 Free PMC article.
-
Modelling of biological age in stable and acute exacerbations of chronic obstructive pulmonary disease.BMC Pulm Med. 2025 Aug 19;25(1):398. doi: 10.1186/s12890-025-03841-4. BMC Pulm Med. 2025. PMID: 40830456 Free PMC article.
-
Association between lung function and exacerbation frequency in patients with COPD.Int J Chron Obstruct Pulmon Dis. 2010 Dec 9;5:435-44. doi: 10.2147/COPD.S13826. Int J Chron Obstruct Pulmon Dis. 2010. PMID: 21191438 Free PMC article.
-
Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: a systematic literature review.Respir Res. 2022 Aug 23;23(1):213. doi: 10.1186/s12931-022-02123-5. Respir Res. 2022. PMID: 35999538 Free PMC article.
References
-
- Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease 2024 report [EB/OL]. (2023-11-13)[2024-12-18]. Available from: https://goldcopd.org/2024-gold-report/. Accesssed June 03, 2025.
-
- Momtazmanesh S, Moghaddam SS, Ghamari S-H, GBD 2019 Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936. doi: 10.1016/j.eclinm.2023.101936 - DOI - PMC - PubMed
-
- WHO. Multimorbidity. Geneva: world health organization. 2016. Available from: http://apps.who.int/iris/handle/10665/252275. Accessed 2003 June 11.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
